


1Department of Pediatrics, Örebro University Hospital, Örebro, 2University Healthcare Research Center, Faculty of Medicine and Health, Örebro University, Örebro, 3Department of Dermatology, Skåne University Hospital, Lund University, Malmö, 4Department of Occupational and Environmental Dermatology, Skåne University Hospital, Malmö, and 5Hospital library, Central Hospital Karlstad, Region of Värmland, Sweden
#These authors contributed equally.
The primary objective of this study was to systematically review and analyse epidemiological studies of the prevalence and incidence of atopic dermatitis (AD) during childhood and adulthood, focusing on data from the 21st century. A systematic search of PubMed, EMBASE and Google (manual search) was performed in June 2019, followed by data abstraction and study quality assessment (Newcastle–Ottawa Scale). Cross-sectional and longitudinal epidemiological studies of individuals with AD (doctor-diagnosed or standardized definition) were included. Of 7,207 references reviewed, 378 moderate/good-quality studies were included: 352 on prevalence of AD and 26 on incidence of AD. In the 21st century, the 1-year prevalence of doctor-diagnosed AD ranged from 1.2% in Asia to 17.1% in Europe in adults, and 0.96% to 22.6% in children in Asia. The 1-year incidence ranged from 10.2 (95% confidence interval (95% CI) 9.9–10.6) in Italy to 95.6 (95% CI 93.4–97.9) per 1,000 person-years in children in Scotland. There were few recent studies on incidence of AD in the 21st century and no studies on adults only; most studies were conducted in Europe and the USA. Epidemiological studies on childhood and adulthood AD in different continents are still needed, especially on the incidence of AD during adulthood.
Key words: systematic review; atopic dermatitis; prevalence; incidence.
Accepted May 7, 2020; Epub ahead of print May 15, 2020
Acta Derm Venereol 2020; 100: adv00160.
Corr: Laura B. von Kobyletzki, Department of Dermatology, Skåne University Hospital, Lund University, SE-205 02 Malmö, Sweden. E-mail: lbkoby@gmail.com
Atopic dermatitis is common, and is often burdensome for the individual. An overview of how often AD occurs is therefore necessary. A systematic review was performed, which included more than 7,000 articles with data from all continents, on children and adults. Each year, up to 17.1% of adults and 22.6% of children were diagnosed with AD; with as many as 9.6% new cases of AD in children. Surprisingly, in adults, studies on new cases were from the 20th century. The results will be useful for patient organizations, physicians, scientists and healthcare planning, especially as new therapies are emerging.
Atopic dermatitis (AD) is a common inflammatory skin disease. AD causes an itchy rash and dry skin and has a substantial impact on quality of life (1, 2). In Europe and the USA, recent data suggests that the prevalence of AD among children is approximately 20% and, among adults, it ranges between 7% and 14%, with substantial variation between countries (1, 3–8).
AD leads to substantial social and financial costs and accounts for the largest global burden of disability owing to skin diseases (9).
The onset of AD occurs during the first years of life in approximately 80% of individuals (10), and that appro-ximately 60% experience remission in adolescence (11). Recent studies indicate evidence of adult-onset AD, but the incidence across different age groups and countries remains unclear (12–14).
Differences in study design and definition of AD contribute to the heterogeneity in reported prevalence and incidence data (15). Differences across studies in factors such as study design, research teams, location, and methods, result in heterogeneity in estimates of the prevalence and incidence of AD, which may underestimate or overestimate the “true” prevalence and incidence of AD in children and adults. Furthermore, AD often features intermittent disease symptoms and signs, which can differ across age groups and skin types.
Knowledge of the prevalence and incidence of AD across different age groups and countries is essential for healthcare planning and patient counselling. Diagnosis based on validated diagnostic criteria, especially physician diagnosis, is often the preferred method. The United Kingdom Working Party diagnostic criteria (UK criteria) are a validated measure for physician assessment of AD and are thus useful (16). Epidemiological data from the 21st century could increase our understanding of the burden of AD.
The primary objective of this study was to systematically review and analyse epidemiological studies of the prevalence and incidence of AD during childhood and adulthood, with a particular focus on publications from 2000 through 2019. Secondary outcomes were the prevalence and incidence across age, sex, decade, and country/region.
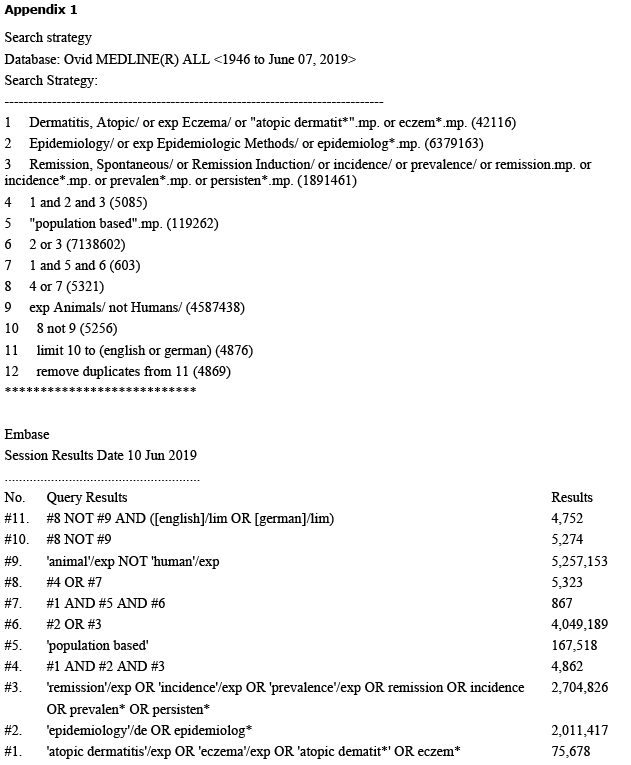
A systematic search of PubMed, EMBASE, and Google (manual search) was performed in June 2019. Pre-defined search terms and MeSH (Medical Subject Heading) headings and keywords were developed in collaboration with a medical librarian. The searches are described in Appendix 1. Reference lists of included studies and conference abstracts were also screened and Google was searched manually for potential additional studies.
Study selection, data abstraction, and quality assessment
The study included cross-sectional and longitudinal epidemiological studies of individuals with AD, diagnosed by a doctor or using a standardized definition, such as the UK criteria for AD or the International Study of Asthma and Allergies in Children (ISAAC) criteria (17). We primarily searched for studies in English and German. Following a manual search, relevant articles in other languages were also included; specifically, one article in Dutch, 8 in French, and one in Spanish. Exclusion criteria were: intervention studies, clinic-based studies, studies on specific exposed populations (e.g. occupations), and studies of patients with hand eczema only. Title, abstract, and full-text screening was perform-ed independently by two authors in order to assess whether the predefined eligibility criteria were met.
Predefined data extraction sheets and quality assessment sheets were used, which included the Newcastle–Ottawa Scale (NOS) for cohort studies and a modified version of the NOS for cross-sectional studies (18). Screening, data extraction, and quality assessment were performed by two authors (LvK, SB), and discrepancies were resolved by author consensus. Corresponding authors of studies were contacted via e-mail when possible to obtain information about prevalence or incidence by sex.
The primary outcome was prevalence (point prevalence, 1-year (y) prevalence, and/or lifetime prevalence) and incidence of AD. Secondary outcomes included the prevalence and incidence of AD across age, sex, decade, and country/region and quality assessment using the NOS. A particular focus was on publications using data from 2000 through 2019.
This review is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (19). When numbers were provided in the original articles but not percentages, then percentages were calculated.
Study selection
The search identified 7,207 abstracts. Of these, 966 articles were selected for full-text review. A manual search and article reference list search identified another 21 studies. Of the articles reviewed, 378 fulfilled the inclusion criteria. In total, 115 of the included studies used data from 2000 onwards. A total of 20 of the studies with data from, and including, 2000 onwards reported 1-year prevalence for doctor-diagnosed AD, and 6 reported incidence for doctor-diagnosed AD. Of the papers included, 337 reported on children and 54 on adults or on both children and adults.
The study flow diagram (Fig. 1) reports article numbers and reasons for exclusion.
Fig. 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram. Results of search strategy. *No assessment of atopic dermatitis (AD): data on asthma, allergic rhinitis or allergy and not specifically on AD.
Study characteristics
The studies identified in the search in June 2019 included data from 1958 to 2017. Of these studies, 200 were conducted in Europe, 122 in Asia, 20 in North America, 20 in South America, 23 in Africa, and 14 in Australia; several articles reported on data from several countries. Study samples were between 108 to more than 30 million individuals. Some studies were conducted on several continents and on both children and adults. For study characteristics, see Supplement 1 (http://lup.lub.lu.se/record/e240247d-7664-4263-9918-3b38e704fd06).
There were 342 cross-sectional studies and 36 longitudinal studies. Twenty-eight studies used a doctor diagnosis drawn from study records or patient records and 2 studies relied on a doctor diagnosis based on both physical examination and questionnaire data.The longitudinal studies often used birth cohorts; the earliest of these started in 1958.
The definition of AD varied, and often the ISAAC criteria were used; only 10 studies used the UK criteria and 11 used the Hanifin & Rajka criteria (20), as described in Supplements 1–7 (available from http://lup.lub.lu.se/record/e240247d-7664-4263-9918-3b38e704fd06).
Prevalence of atopic dermatitis
The results for prevalence are presented in Tables I and II and Supplements 2–7 (available from http://lup.lub.lu.se/record/e240247d-7664-4263-9918-3b38e704fd06).
Table I. Doctor-diagnosed 1-year prevalence of atopic dermatitis (AD) in children assessed in the year 2000 or later by continents
Table II. Doctor-diagnosed 1-year prevalence of atopic dermatitis (AD) in adults assessed in the year 2000 or later by continents
Studies on children and on both children and adults: all data (1958–2018). The overall point prevalence of AD symptoms in children ranged from 1.7% to 32.8% (21–25). The 1-year prevalence of AD symptoms varied from 0.7% in children and adults in Ethiopia (26), to 2.0% in children in Urumqi (27), and 22.7% in Kuwait (28). The 1-year prevalence in children based on doctor diagnosis of AD ranged from 0.96% to 22.6% (21–25).
The lifetime prevalence of AD varied from 1.2% in Turkey in children aged 7–12 years (132), the same lifetime prevalence of 1.2% was reported in Ethiopia (26) in children and adults with a mean age of approximately 22–23 years, and 36.2% in Beijing (27); the age at assessment of lifetime prevalence was 6–7 years. Lifetime prevalence of doctor-diagnosed AD assessed at age 6–7 years was 1.4% in Lithuania and 36.2% in Beijing (27, 29).
Studies on adults: all data (1958–2018). In adults, the overall point prevalence of AD symptoms ranged from 1.2% to 9.7% (1, 30). The 1-year prevalence of AD symptoms varied from 1.3% in Germany to 22.7% in Kuwait (28, 31), and the 1-year prevalence based on doctor diagnosis ranged from 1.2% to 17.1% (1, 32).
The lifetime prevalence of AD ranged from 1.7% to 17.7% in Kuwait; the age at assessment of lifetime prevalence was 18–26 years. The prevalence of AD in Scandinavia between ages 0–29 years was 34.1%; the lifetime prevalence of doctor-diagnosed AD was 14.6% to 20.2% in Kuwait; the age at assessment of lifetime prevalence was 18–26 years (1, 28, 31, 33).
Studies of 21st century data for children and adults. For children, the point prevalence ranged from 0% in Nigeria to 18.2% in Turkey (39, 40). For adults, it varied from 0.64%–0.9% in Israel to 9.7% in Denmark in 2010 (1, 41). For children, the 1-year symptom prevalence ranged from 4.1% to 22.7% and for adults from 7.3% to 22.7% (28, 42, 43). The 1-year prevalence of doctor-diagnosed AD ranged from 1.2% in Asia to 17.1% in Europe in adults, and from 0.96% to 22.6% in children in Asia (1, 32, 34–36). For children, the lifetime symptom prevalence ranged from 4.4% to 17.7% assessed at age 7–15 years, and for adults ranged from 3.0% to 17.7% (28, 31, 44). For children, the lifetime prevalence of doctor-diagnosed AD ranged from 4.7% to 20.2% assessed at age 7–15 years and for adults ranged from 17.6% to 20.2% (28, 31, 45).
Trends by continent: 21st century data. In Asia, studies reporting repeated measures indicated higher proportions of AD in the 21st century. For example, Liao et al. (46) assessed the prevalence of parent-reported AD symptoms in 2002 and 2007 in 6–8-year-olds in Taiwan and reported an increase from 5.8% to 7.7%, and an increase in lifetime prevalence of doctor-diagnosed AD from 18.0% to 23.9%. In the 21st century in Europe and North America there was no specific trend and data seemed stable for studies that reported repeated measures (46–53).
Trends by continent: all data (1958–2018). As shown in Supplements 2–4 (available from http://lup.lub.lu.se/record/e240247d-7664-4263-9918-3b38e704fd06), in Africa, prevalence of AD has generally increased; some studies that reported repeated measures of AD across different years confirm this trend (54–56), although one study from Nigeria reported the opposite trend (57). In Asia, some studies suggest an increasing prevalence (46, 58–60), but the results are mixed (61–63) and prevalence of AD was generally lower compared with other regions such as Europe. In the USA, the prevalence reported was somewhat higher in the 21st century compared with the 20th century; however, the few studies reporting repeated measures suggested no clear trend (64–66). In Europe, most studies reported an increasing incidence and prevalence in the 21st century compared with the 20th century and studies reporting repeated measures also suggest an increase in AD (67–74), although other studies found no increase (53, 75). In Australia, most studies suggested a higher prevalence in recent years compared with the 20th century, and this was confirmed in most of the repeated measures studies (76, 77).
Prevalence by sex: all data (1958–2018). Of all studies, 54 reported on the prevalence or incidence of AD by sex. The 1-year prevalence of AD and lifetime prevalence of doctor-diagnosed AD was higher in females (range 0.6–24.3%; 1.0–35.5%, respectively) than in males (range 0.8–17.6%; 1.4–37.3%, respectively) in most studies (Supplements 5–7; http://lup.lub.lu.se/record/e240247d-7664-4263-9918-3b38e704fd06), and this was consistent across different continents, although a higher prevalence in males was also reported (72).
The point prevalence in children assessed in good-quality studies was 24% in females compared with 35% in males at age up to 1 year; in schoolchildren the proportions were 11.1% and 8.1%, respectively (78, 79). One good-quality study that used the NOS assessment in adolescents aged 12–14 years showed a 1-year symptom prevalence for girls of 9.64% and for boys of 17.10% (80). In adults, the point prevalence was 10.2% in females and 5.8% in males (28). The 1-year symptom prevalence in female adults was 13.1% (95% confidence intervals [CI] 12.4–13.8) and in males 10.8% (95% CI 2.4–13.8).
Prevalence by age and continent: all data (1958–2018). The prevalence of AD was stable across age groups and across populations. There were no differences in prevalence across continents; for example, prevalence of AD was high in both Sweden and Africa. However, lower prevalence was observed in China, central Asia, and eastern Europe. There was no clear trend regarding age groups. For example, Burr et al. (82) reported a 1-year prevalence lower than 10% for children, similar to Nissen et al. (83), but higher prevalences were also reported and similar numbers reported for adults by Williams & Strachan (84). However, when considering the range of reported 1-year prevalence in the 21st century, children showed the highest prevalence (22.6%) (28, 36, 81–84).
Study design and assessment methods
There was heterogeneity across study designs and study populations and therefore a meta-analysis was not performed. Studies using signs of AD (ISAAC) reported a higher prevalence of AD than those using physician diagnosis. The number of times AD was measured per study period did not significantly affect the reported prevalence of AD.
Incidence of atopic dermatitis
Atopic dermatitis incidence for 21st century data. The incidence of AD was reported in 17 studies; of these, 6 studies were conducted in the 21st century (Table III). The 1-year incidence ranged from 10.2 (95% confidence interval (CI) 9.9–10.6) in Italy to 95.6 (CI 93.4–97.9) per 1,000 person-years in children in Scotland. The incidence of AD in adults was 7.41 (6.27–8.74) per 1,000 person years in 1968 (85).
Table III. Summary of study results regarding incidence of atopic dermatitis in children and adults from the year 2000 and onwards
Atopic dermatitis incidence for all data (1958–2018). In all included studies, the highest incidence of AD occurred during infancy and the incidence was also high in early childhood. For example, Nissen et al. (83) reported the highest incidence of AD during the first 18 months of life, von Kobyletzki et al. (11) reported that approximately 80% of children with AD had disease onset during infancy, and Williams et al. (84) reported that 66% had disease onset by the age of 7 years. Ballardini et al. (81) found that, between age 0–12 years, the proportion of “new” incident cases in the last 12 months in Stockholm, Sweden, was 53% of all prevalent cases. How-ever, a considerable incidence was also reported during adolescence and adulthood. The reported proportion of adult-onset AD was 8.0% in Germany at age 28–30 years (1, 52, 86–90).
Study quality
The study quality ranged from moderate to good, as shown in Supplement 2 (http://lup.lub.lu.se/record/e240247d-7664-4263-9918-3b38e704fd06). One study reported on infant-onset AD and this may have excluded prevalent AD diagnosed during later childhood or adulthood.
Some studies, such as the COPSAC study, included high-risk infants in addition to the “general population”, thus potentially overestimating the prevalence and incidence of AD (91).
This was a systematic review of 378 cross-sectional and birth cohort studies of several million individuals from all continents. The findings indicate a high prevalence of AD across continents.
The studies were heterogeneous, which made it difficult to compare the epidemiology of AD in different settings. Several different diagnostic criteria were used and the study designs differed. Furthermore, the appearance, knowledge of, and definition of AD may differ across continents, cultures, and time periods. This makes comparisons between geographical regions and time periods difficult. The study size also varied considerably. However, with this in mind, the results suggest that there are steady prevalence estimates across different age groups.
There were more studies on children, and doctor-diagnosed 1-year prevalence of AD was seldom assessed in Africa, South America, and Australia. This may be partly explained by differences in healthcare, as the European studies often used general practitioner datasets or insurance data.
The reported prevalence of AD was usually higher during the 21st century than the 20th century, especially in Africa and even in Europe. The data for Asia were more heterogeneous. There was a high prevalence of AD in children and adults. The high prevalence of AD in adults could be explained by high persistence or adult onset of AD. Some studies suggested a higher prevalence of AD for females than for males across all ages; however, there were conflicting results regarding sex differences. A higher prevalence of AD in males may be a result of surveillance bias in some settings (72). Interestingly, the incidence was high in all age groups, and more studies are needed on the definition and associated factors of adult incident AD.
Strengths and limitations
No articles were excluded from the review because of language restrictions, and the search strategy was designed to detect all relevant studies. However, it is possible that some relevant studies were missed. The definitions of AD may have changed over the decades; however, the trends in data using doctor-diagnosed AD, self-reported AD using ISAAC criteria, and otherwise-reported AD were quite stable.
Some diagnostic criteria included infant onset of disease and thus some cases of AD with onset later than infancy might have been missed (92). As the symptoms and signs of AD may vary across age groups and skin types, using the same diagnostic criteria for different groups of patients may overestimate or underestimate AD in some groups. However, comparison of data using similar diagnostic criteria is very useful, and validated self-report measures to diagnose AD are needed.
Although similar diagnostic criteria were used in some studies, like the ISAAC or adapted ISAAC criteria, differences in study design and slight differences in the questionnaires used made it difficult to summarize the data. In contrast, the study by Williams et al. compared the prevalence of AD symptoms in 56 countries using a similar study design and method (93).
This systematic review included a comprehensive search and a critical assessment of the reviewed studies. The findings report data from representative population-based epidemiological studies, including those with large representative cohorts, data from several decades, and data from all continents. The study thus reports on findings in highly diverse settings and populations.
However, some included studies were designed to assess the prevalence and incidence of AD, whereas others reported on AD as a secondary outcome. The definition of AD is important, as it affects the reported proportions; it is possible that other forms of dermatitis were included. Most epidemiological studies had no information on treatment, which might have influenced disease symptoms and reported prevalence of AD symptoms.
Many studies lacked data on participation rate, and only a few studies reported data on socioeconomic position. It is possible that individuals with AD who had higher socioeconomic status were more likely to participate.
The studies in this review included data from 1958 until 2017. The changes in prevalence and incidence may reflect changes in disease patterns and prevalence of risk factors; however, the fact that studies used different methods of AD assessment should be kept in mind. This review reports point prevalence, 1-year prevalence, and lifetime prevalence. This comprehensive reporting may be useful, as prevalence of AD can show seasonal variations.
Comparison with other studies
The results of this study compare well with results from a systematic review using ISAAC data with a mean 12-month prevalence of 7.9% at age 6–7 years and 7.3% at age 13–14 years. The present data are also in accord with data from ISAAC studies suggesting that there is no clear pattern of prevalence of AD across continents (17). The results are in line with studies suggesting a lower prevalence in the 20th century than in the 21st century (94, 95). In a systematic review by Abuabara et al. (96), a prevalence of AD for adolescents/young adults and children was similar to our findings. A review by Pols et al. (95) reported that the assessed prevalence of AD may vary according to diagnostic methods. More studies are needed using the same validated diagnostic tools and a similar study design. There are more studies on the epidemiology of AD in Europe and the USA; a comprehensive worldwide assessment is needed.
There is also a lack of incidence studies. An understanding of incidence is important for the understanding of disease mechanisms (97). Changes in incidence can even suggest risk factors that need targeting. Most studies use questionnaire data to assess the prevalence of AD, and validated diagnostic criteria are important. The ISAAC criteria and the UK criteria are validated and used worldwide, which permits data comparisons. Further standardization and validation for self-reported assessment of AD may be useful. The results of this study have relevance for healthcare planning and patient counselling.
Below, the 14 references appearing in Tables I–III of this papers are numbered in accordance with the complete list of references also appearing in the supplements shown at: http://lup.lub.lu.se/record/e240247d-7664-4263-9918-3b38e704fd06.
Conclusion
As assessed by both patients and physicians, AD is a common disorder that has increased in most continents and reached a stable plateau in Europe and North America. There are only a few recent studies on the incidence of AD in the 21st century and no studies on adults only; most studies have been conducted in Europe and the USA. More epidemiological studies on childhood and adulthood AD in different continents are needed, especially on the incidence of AD during adulthood. However, assessment of AD must be more standardized across cultures in order to improve future epidemiological studies.
The authors thank Diane Williams, PhD, from Edanz Group (www.edanzediting.com/ac) for editing a draft of this manuscript.
(complete list of references also appearing in the supplements shown at: http://lup.lub.lu.se/record/e240247d-7664-4263-9918-3b38e704fd06.)


 Click to show fullsize
Click to show fullsize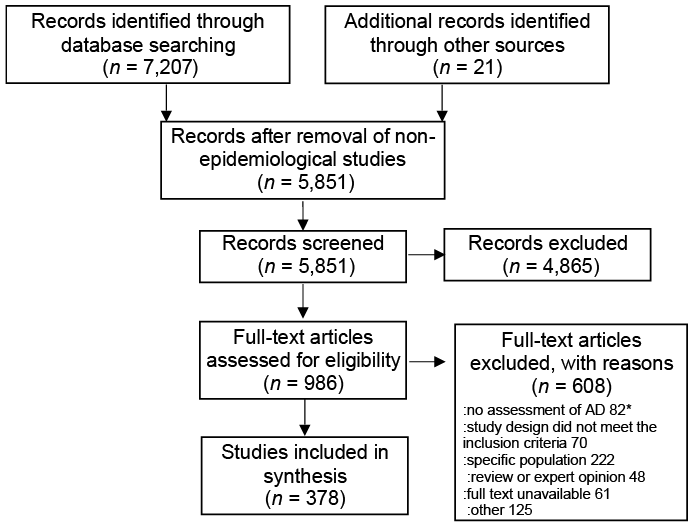 Click to show fullsize
Click to show fullsize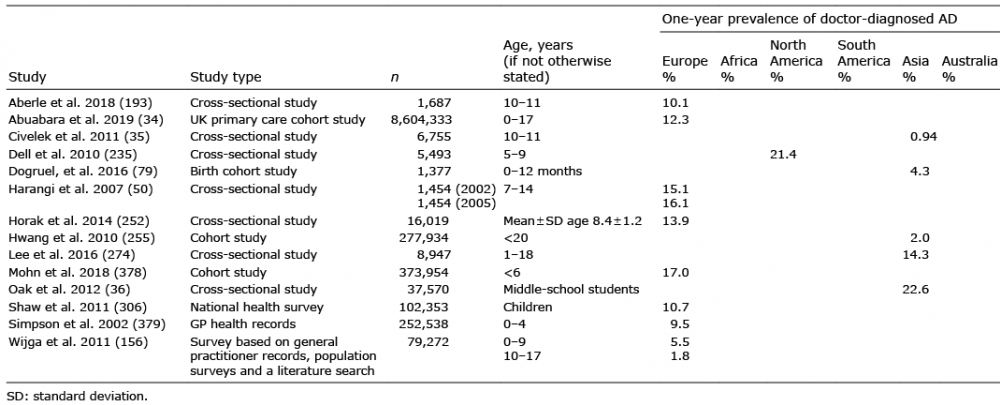 Click to show fullsize
Click to show fullsize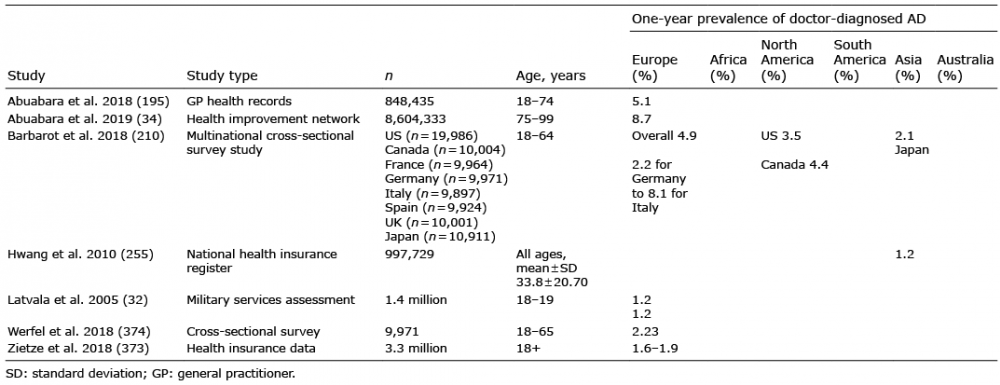 Click to show fullsize
Click to show fullsize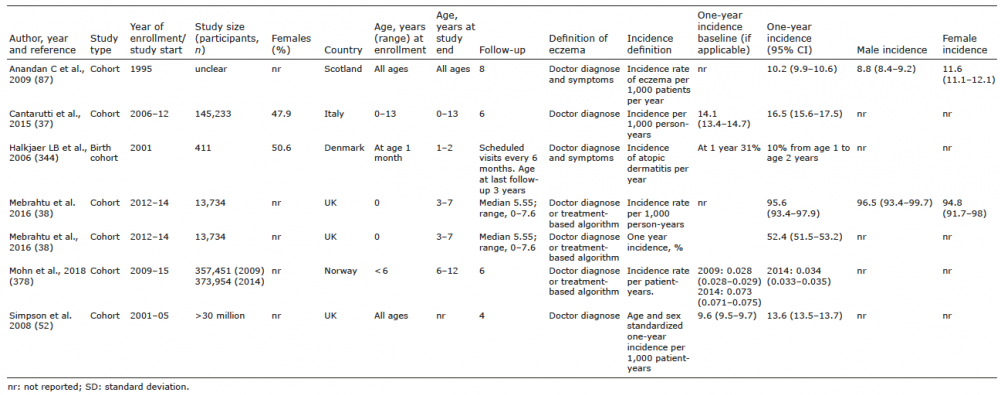 Click to show fullsize
Click to show fullsize