


1Dermatology Department, Bellinzona Regional Hospital, Bellinzona, and 2Istituto Cantonale di Patologia, Locarno, Switzerland. E-mail: caroline.delorenzi@eoc.ch
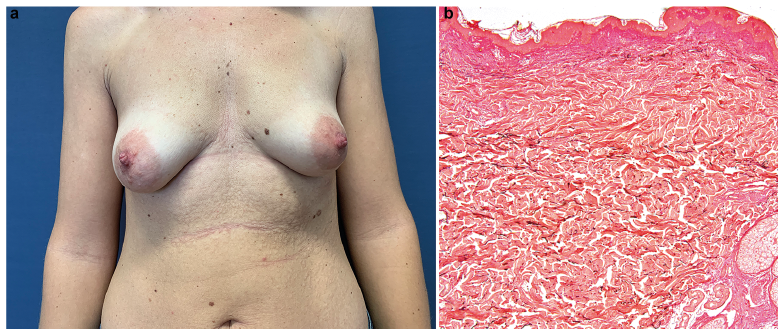
A 38-year-old woman was referred to our dermatology clinic for a second opinion regarding skin lesions. The lesions had first appeared at the age of 34 years, on her trunk then spread to her back, initially as red papules, leaving wrinkling skin. The patient was asymptomatic and did not present any other general symptoms. Her medical history was unremarkable except for an assisted pregnancy. She was not taking any medication. She had a history of going to tanning salons. Her familial history was negative for skin conditions. On clinical examination, she presented widespread papules and plaques, with wrinkling and mild protrusion from the surface of the skin, distributed over the trunk and abdomen (Fig. 1a) and back. Histologically, Verhoeff-Van Gieson staining revealed mid and profound dermal loss of elastic fibres (Fig. 1b). Blood testing revealed anti-thyroglobulin antibodies at 6.7 IU/ml (normal < 4.1 IU/ml); other routine analyses (thyroid-stimulating hormone, immunology test-ing, and proteins electrophoresis) were in the normal range.
What is your diagnosis? See next page for answer.
Fig. 1. (a) Papules and plaques, with wrinkling and mild protrusion on the abdomen. (b) Histology showing mild and profund dermal loss of elastic fibres on Verhoeff-Van Gieson staining. Original magnification, ×5.
Acta Derm Venereol 2020; 100: adv00190.
Diagnosis: Mid-dermal elastolysis
Clinical presentation and histology in this case were compatible with a type II mid-dermal elastolysis (MDE). MDE is a rare acquired elastic tissue disease, first described by Shelley & Wood in 1977 (1–3). Clinically, it predominantly affects the trunk, back, shoulders and upper extremities, with a symmetrical distribution (1, 2, 4, 5). The palms, soles and faces are spared (1). Three clinical variants are described: type I MDE consists of well-defined patches of fine wrinkles arranged in parallel to the skin cleavage line, type II MDE consists of soft perifollicular papular protrusions. They predominantly affect Caucasian females (1, 2, 4). Type III MDE consists of reticulate erythema on sun-exposed areas and has a male predominance (1, 2, 4). Burning symptoms and/or erythema, urticarial papules or plaques can precede the wrinkled plaques in 50% of cases (1–5).
The pathogenesis of MDE is obscure. Overexpression of metalloproteinases-1 and -9 responsible for the elastolytic activity and reduction in protein expression of LOXL2, implicated in the homeostasis of elastic fibres, appeared to be important pathogenic factors (6). Currently it is not clear if ultraviolet radiation or hormones play a role in the changes in metalloproteinases (1, 4, 7). In addition, associated factors have been described, such as systemic lupus ery-thematosus, rheumatoid arthritis, Hashimoto’s thyroiditis, Grave’s disease, type 1 diabetes, granuloma annulare, urticaria, pregnancy, immune reconstitution inflammatory syndrome, mammoplasty, but also serological finding, such as false-positive serology for Borrelia burgdorferi, positive antinuclear antibodies, protein S deficiency and anti-phospholipid antibodies (1–3, 5, 7–9). An immune process against elastic fibres is thus suggested in the pathogenesis of MDE, the disease being described in association with different inflammatory and immune diseases (1, 2, 7).
A band-like or focal loss of elastic fibres along the mid-dermis, seen on Van Gieson or orcein staining and sparing the papillary and lower reticular dermis, is the characteristic histopathological finding; haematoxylin and eosin stainings are frequently normal (1, 2, 4, 5).
Differential diagnosis includes anetoderma, cutis laxa, perifollicular elastolysis, pseudoxanthoma elasticum-like papillary dermal elastolysis and annular elastolytic giant cell granuloma (4, 5).
Different treatments have been reported in the literature, with no clear benefit. Topical therapies, such as steroids, soybean extract, and eicosapentanoic acid (or tretinoin, and systemic therapies, such as steroids, colchicine, chloroquine, clofazimine, and dapsone, have been described (1–3, 5, 7). Management is, nevertheless, challenging as there is no consensus and due to the cosmetic implications of MDE.


 Click to show fullsize
Click to show fullsize