


Department of Dermatology, Fukushima Medical University, Hikarigaoka 1, Fukushima 960-1295, Japan. E-mail: ysmyk081@fmu.ac.jp
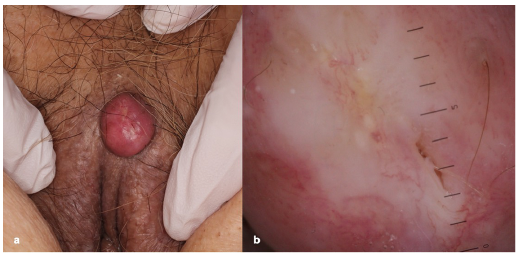
An 87-year-old woman was referred to our department with vulvar lesion of 1-month duration. She had developed a small nodule on her vulva with mild pruritus, and had routinely scratched the area. The nodule had rapidly increased in size. Her medical history included cerebral infarction, hypertension, and osteoporosis. Physical examination revealed a 15-mm, firm, exophytic, dome-shaped, red nodule with a small ulcer on the upper left edge of her labia majora (Fig. 1a). Dermoscopy revealed pink-white structureless areas and linear-irregular vessels (Fig. 1b), and there was hair growth on the surface of the lesion. An excisional biopsy with 2-mm margins was performed.
What is your diagnosis? See next page for answer.
Fig. 1. Clinical findings. (a) A 15-mm, clearly marginated, firm, exophytic, dome-shaped, red nodule with a small ulcer on the upper left edge of the labia majora. (b) Dermoscopy showed pink-white structureless areas and linear-irregular vessels. There was hair growth on the surface of the lesion (scale: 1 mm).
Acta Derm Venereol 2020; 100: adv00185.
Diagnosis: Vulvar keratoacanthoma
Histopathological examination revealed symmetrical, cup-shaped exophytic and endophytic proliferation of squamous epithelium with a central keratin-filled crater (Fig. 2a). The proliferating squamous cells were eosinophilic, glassy in appearance, and only rare mitotic figures or cytological atypia were observed (Fig. 2b). Thereafter, no local recurrence was observed during the 2-year follow-up.
Vulvar keratoacanthoma is very rare and, to the best of our knowledge, there have only been 6 cases reported previously in the English literature (1–5). Including the current case, the clinical characteristics of all 7 cases are shown in Table I. The median age of the 7 cases is 54 years, ranging from 33 to 87 years. The patient in the current report, at 87 years of age, is the oldest subject reported to date. The onset sites were on the labia majora (n = 5) and clitoris (n = 2), and the clinical appearance of most cases was expressed as a raised nodule of approximately 1 cm. In one case the lesion was characterized by a central crater and in 2 cases by a central ulcer; however, the other 4 cases had no craters or ulcers. None of the reported cases had hyperkeratosis, and the duration of the lesions ranged from 4 weeks to a few months, during which each lesion proliferated rapidly. There was no mention of a tendency to spontaneous regression, because excisional biopsy was performed in all cases. There were no cases of recurrence. Two cases were diagnosed as well-differentiated squamous cell carcinoma after partial biopsy (1, 3).
In the present case, the patient noticed a vulvar nodule with pruritus, which enlarged rapidly during scratching; however, the triggering factor remains unclear. Keratoacanthoma is clinically characterized by a well-circumscribed nodule with a central keratotic plug. In contrast, the current case presented with a pink-coloured nodule with a smooth surface. Keratoacanthoma involving the vulva assumes an atypical clinical appearance, differing from those arising on other sites, such as a lower keratotic tendency. In the case of a rapidly growing nodule on the vulva, kerato-acanthoma should be included in the differential diagnosis of malignant tumours, such as squamous cell carcinoma.
Dermoscopy of keratoacanthoma shares some features with squamous cell carcinoma and cannot be used to clearly differentiate these entities (6). Keratin and white circles with dot vessels are useful to differentiate keratoacanthoma and squamous cell carcinoma from other rapidly-growing crateriform nodules (7).
Keratoacanthoma is a common tumour that is thought to derive from hair follicles. The majority of cases involve the face, and vulvar involvement is rare. We here report the first case of vulvar keratoacanthoma from Japan.
Fig. 2. Histopathology. (a) Histological features of the excision specimen showed symmetrical, cup-shaped exophytic and endophytic proliferation of squamous epithelium with a central keratin-filled crater (haematoxylin-eosin (H&E), original magnification ×12.5). (b) Histological features of the nodule on the skin showed small aggregates of atypical cells in granulation tissue (H&E, original magnification ×100).
Table I. Vulvar keratoacanthoma reported in the English literature


 Click to show fullsize
Click to show fullsize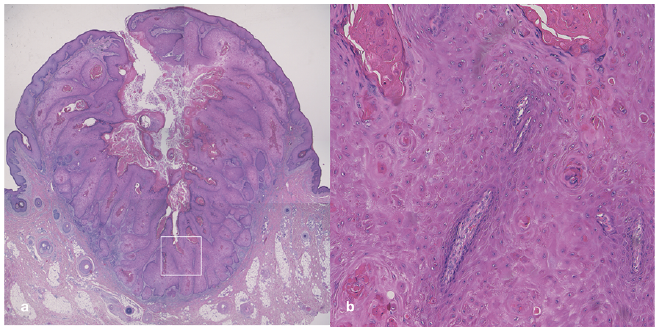 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize