


1Department of Dermatology, Amsterdam Public Health, Infection and Immunity, Amsterdam UMC, University of Amsterdam, Amsterdam, 2Department of Dermatology, Sint Antonius Hospital, Nieuwegein, 3Knowledge Institute of the Dutch Association of Medical Specialists, Utrecht, 4Skin patients, Nieuwegein, 5Netherlands Patients Federation, Utrecht, and 6Dutch Association for People with Atopic Dermatitis, Nijkerk, The Netherlands
#Both authors contributed equally and share first authorship. *Contributing patients/patient representatives.
In shared decision making (SDM) patients and physicians make treatment decisions together based on the best available evidence and the values and preferences of patients. SDM is very suitable for use in dermatological practice, but is infrequently applied by dermatologists. To support the application of SDM in dermatology we developed Decision Cards: 1-page overviews of possible treatment options, for use during a patient–physician consultation. Decision Cards provide answers to patients’ most frequently asked questions, based on (inter)national guidelines, Summary of Product Characteristics, relevant literature, and clinical expertise. Three evidence-based Decision Cards were developed: 1 for biologicals or apremilast in psoriasis, and 2 for atopic eczema (1 for topical, photo- or systemic therapy, and 1 for systemic therapy only). More cards for psoriasis are currently in development. Patients, dermatologists and researchers collaborated in the development of the Decision Cards. This paper shares the framework used for the development of the Decision Cards, in order to support others in the development process.
Key words: shared decision making; encounter decision aids; psoriasis; atopic eczema; decision card.
Accepted Aug 13, 2020; Epub ahead of print Aug 19, 2020
Acta Derm Venereol 2020; 100: adv00337.
doi: 10.2340/00015555-3614
Corr: Francisca M. Vermeulen and Gayle E. van der Kraaij, Department of Dermatology, Amsterdam University Medical Centres, University of Amsterdam, Meibergdreef 9, NL-1105 AZ Amsterdam, The Netherlands. E-mail: f.m.vermeulen@amsterdamumc.nl; g.e.vanderkraaij@ amsterdamumc.nl
In shared decision making, patients and doctors share the best available evidence to find a treatment that best suits the patients’ values and preferences. This process improves patients’ knowledge and the likelihood of patients making decisions that are more congruent with their values, doctor– patient communication, and satisfaction with the treatment decision/decision making process. This paper describes the development of 3 Decision Cards to support this process: one for biologicals or apremilast in psoriasis, one for topical, photo- or systemic therapy in atopic eczema, and one for systemic therapy in atopic eczema. A framework that others can use to develop Decision Cards is presented.
Shared decision making (SDM) can be defined as an approach in which physicians and patients share the best available evidence when faced with the task of making decisions, in order to choose the therapy that best suits a patient’s values, preferences and needs (1).
Tan et al. (2) and Anstey & Edwards (3) wrote articles advocating more integration of SDM in dermatology. Many skin diseases have multiple treatment options, usually without a single best treatment. The best treatment depends on disease aspects (e.g. extent and location of the lesions), patient aspects (e.g. comorbidity, co-medication and physical and emotional burden of the disease), and patient preferences (e.g. the frequency and route of administration, number of needed hospital visits or the need for controls). These aspects can vary between patients and in the same patient over time. Such preference-sensitive treatment decisions are most suitable for SDM (4).
Three steps have been proposed to apply SDM during a consultation: (i) acknowledge that a treatment decision has to be made and explore what role the patient wants in this decision making process, (ii) compare treatment options and discuss the benefits and harms of these options, (iii) make a treatment decision that best suits the patient’s expectations, needs and lifestyle, guided by the experience of the healthcare team (5).
Patient decision aids (PDAs) are tools to support patients in the decision-making process, by providing information about treatment options and helping patients to identify their values. Encounter decision aids (EDAs) are PDAs developed for use during a consultation (6, 7).
The use of a decision aid improves patients’ knowledge and the likelihood of patients making decisions more congruent with their values (8). It improves doctor– patient communication and satisfaction with the treatment decision and decision-making process, compared with usual care (8). Use of a decision aid may enhance treatment compliance, although studies report different outcomes on this subject (8).
The challenge in the development of decision aids is to provide scientifically correct information, which is helpful and understandable for patients. They are therefore preferably developed according to an established format. We developed Decision Cards; 1-page EDAs with an overview of different treatment options based on the questions most frequently asked by patients. They are similar to Option Grids, which have been designed and studied extensively by Glynn Elwyn’s group (9–12), and make the treatment options easy to discuss because they are standardized and visually displayed (13). Decision Cards are preferably read by patients and physicians together (although patients can also take them home, as long as they engage in the decision making process), and support the discussion of individual patient’s values and preferences, which are therefore only partly incorporated on the cards (9, 14).
To date, no Option Grids or Decision Cards are available in Dutch for any dermatological diseases, nor are such tools available in English for atopic eczema (AE). Since Decision Cards are designed for patients, it is important that they are available in the native language of a patient, and suitable for daily practice in a specific country.
It was decided to develop Decision Cards for psoriasis and AE, since treatment decisions for these diseases are preference-sensitive, many treatment options are available for these diseases, and because psoriasis and AE are common, hence many patients could benefit. This paper describes the framework used to develop the Decision Cards. This framework can be used as an example for the development of EDAs for other dermatological diseases.
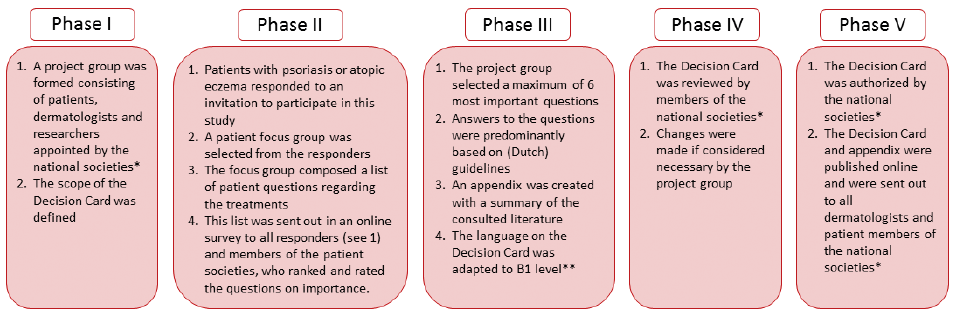
For the development of the Decision Cards a previously established framework was used, in which a clear order of consecutive steps was provided (Fig. 1) (15). This framework complies with the Dutch Protocol for the development of decision aids with guidelines (16), and was developed by the Knowledge Institute of the Dutch Association of Medical Specialists and the Netherlands Patients Federation. Both have been initiators for the development of Decision Cards for multiple diseases. The format was inspired by that of the Dartmouth Institute for Option Grids (not published). The development and usage of Option Grids have been investigated for many years, but its trademark restrains the development of Option Grids by other researchers (9–12).
Fig. 1. Summary of the framework used for the development of a Decision Card. *Dutch National Society for Dermatology and Venereology and patient societies Skin patients the Netherlands and Dutch Association for People with Atopic Dermatitis. **According to the Common European Framework of Reference for Languages.
During the first phase, 2 project groups were formed; 1 for the development of a psoriasis Decision Card and 1 for the AE Decision Cards. Both project groups consisted of dermatologists affiliated with the Dutch National Society for Dermatology and Venereology (NVDV), patients, patient representatives of the national dermatology patient association (Skin Patients the Netherlands and Association for People with Atopic Dermatitis), researchers and project advisors experienced in the development of Decision Cards.
A Decision Card contains a maximum of 6 treatments due to the limited amount of space available (1 side of standard size A4 paper) (13). The project groups therefore defined a specific treatment category (e.g. systemic or topical therapies) and patient group (e.g. adults or children) per Decision Card. The project group selected treatment categories for which the need for more information on the treatment decision was most needed. Only treatments currently captured by the Dutch national guidelines were eligible.
In the 2nd phase, an invitation was sent via email to a cohort of patients with psoriasis and patients with AE. Of those who were willing to participate in the project, a selection was made for participation in a focus group, with the aim of recruiting a group of equal distribution in terms of age, sex, residence, education level and expertise with multiple treatments. Three focus groups, comprising 5 patients with psoriasis, 8 with AE for the first AE Decision Card, and 4 with AE for the 2nd AE Decision Card composed a list of important questions regarding the treatments.
Next, the project group added more questions based on their clinical expertise. An online survey with the complete list of questions was then sent to all psoriasis and AE patients in the cohort, members of the national patient societies, and a link to the survey was placed on the patient societies’ websites. In this survey, patients were asked to judge the questions in 2 different ways:
In the 3rd phase, a maximum of 6 most important questions were selected based on the patient surveys. If questions did not make this cut-off, but were often encountered in clinical practice according to the dermatologists, attempts were then made to merge them with other, already included, questions. In order to formulate answers to these questions, evidence from (inter)national guidelines (from the Netherlands (17, 18), the UK (19), the USA (20, 21) and the European Dermatology Forum (22, 23)) and summary of product characteristics (SmPC) texts were used. In case of discrepancies between guidelines, the national guideline was followed. If the consulted guidelines did not provide the answers, recent systematic reviews, meta-analyses and other (preferably randomized controlled) studies were consulted. Only if necessary, answers were based on expert opinions. Appendices were created containing a summary of the available and consulted literature and the rationale as to why certain information was or was not selected to be used for the answers on the Decision Cards (24–26).
In order to make the Decision Cards as accessible as possible to all patient groups the language used on the Decision Cards was adapted to B1 level according to the Common European Framework of Reference for Languages (27). After finalizing the first draft of the Decision Cards, members of the NVDV and the Dutch patient societies for psoriasis and AE were invited to give feedback (4th phase). In addition to the original framework, the Association Innovative Medicines (the industry association for the Dutch branches of innovative pharmaceutical companies) was invited to provide feedback. The suggestions received for modifications were then re-evaluated by the project group and, only if considered necessary, the answers on the Decision Cards were adjusted. The reasons for or against implementing the suggestions were collected and summarized in the appendix of the corresponding Decision Card. After this last step the Decision Cards were finalized and sent out to the NVDV and patient societies for approval and authorization (5th phase). Finally, the Decision Cards were published online at https://consultkaart.nl.
The Decision Cards were linked to the national guidelines so that any updates to the guidelines will be followed by an update of the Decision Cards.
The project group for the psoriasis Decision Card comprised 1 dermatologist, 1 dermatology researcher, 2 patient representatives and 1 project advisor. The project group for the 2 AE Decision Cards comprised 2 dermatologists, 1 dermatology researcher, 3 patient representatives and 1 project advisor.
Three Decision Cards were developed (see Tables I–III). For psoriasis, 1 card was developed for biologics or apremilast in psoriasis vulgaris, as this is the most frequently encountered treatment decision in our (third-line) hospital. For AE 2 cards were developed: one for systemic medication in AE (AE I) and one for different types of treatment in AE (topical, phototherapy or systemic therapy, AE II). All 3 Decision Cards were designed for adult patients.
Table I. Decision Card: “Moderate to severe psoriasis: a biologic or apremilast?”
Table II. Decision Card: “Atopic eczema: treatment options for systemic drugs in adults. (AE I)”
Table III. Decision Card: ‘Atopic eczema: treatment options in adults. (AE II)’
In February and March 2017, online surveys with the proposed questions for the psoriasis and AE I Decision Cards were carried out. The survey for Decision Card AE II followed in August and September 2017. Thirty-four patients with psoriasis, 76 (AE I) and 60 (AE II) patients with AE completed the surveys. The characteristics of the patients are described in Table IV. The most important questions, including the mean rating score (0–10) and weighted ranking, are described per survey in Tables SI, SII, SIII.
Table IV. Characteristics of the patients participating in the surveys
For psoriasis the selected questions were:
For AE I the questions were:
For AE II the questions were:
In chronic illnesses, such as psoriasis and AE, it is especially important for patients to adopt a more active role in decision making, as, throughout the course of the disease, multiple treatment decisions need to be made (3, 29). The need for decision aids in dermatology, and especially short and feasible decision aids for busy clinicians, was previously indicated by Tan et al. (2), and is also highlighted by research that has shown time-constraints are one of the most important perceived barriers for physicians for the application of SDM (30). Decision Cards are compact tools and provide the most important information to make comparisons at a glance, which is sometimes all that is needed to make a decision (1–3, 13). We therefore believe that Decision Cards are useful support tools to improve SDM in the dermatological setting, and are optimistic that they will find their way into daily practice. We hope that, by sharing our experience, others will be able to develop Decision Cards to further enhance SDM.
Two other EDAs for dermatological diseases could be found. One EDA for psoriasis was presented in the British Association of Dermatologists (BAD) guidelines for biologic therapy for psoriasis 2017 (19). The treatments discussed in this EDA are slightly different, since ixekizumab was discussed and apremilast was not. Also, more and slightly different questions are answered: start dosages are not discussed; effectiveness is registered as PASI 90 instead of PASI 75; drug survival after one year instead of 3 years is mentioned; and side-effects causing cessation of the treatment or admission to hospital due to infection are provided. Another EDA was found for actinic keratosis, but no development methods were reported (31).
Strengths and limitations
The Decision Cards provided in this study were based on the previously described framework (15), which was based on the format of the Dartmouth Institute, and has been used previously for many Decision Cards. Since the Knowledge Institute successfully developed multiple Decision Cards, expertise from their advisors was beneficial for the development of our cards. Because the questions on the Decision Cards were defined by patients as most important, they provide relevant information for patients when facing a treatment decision. Data used to answer these questions were derived from (inter)national guidelines, systematic reviews, international SmPC texts and, if necessary, primary research and clinical expertise. Relevant stakeholders, affiliated to dermatological, pharmaceutical and patient organizations, were involved (either in the development phase or in the review phase), which creates a good support base for the implementation and use of the Decision Cards. To provide transparency, for each Decision Card an appendix was made in which the quality of evidence of the consulted literature can be found. Because the cards are linked to the national guidelines, updates of the guidelines will guarantee updates of the Decision Cards. Since the Decision Cards are in Dutch and the language was adapted to the B1 level according to the Common European Framework of Reference for Languages, the Decision Cards will be useful for many psoriasis and AE patients in the Netherlands. For the purpose of this article, English versions of the Decision Cards are provided, which are loosely translated from the Dutch Decision Cards.
A few limitations need to be mentioned. Due to the limited space on a Decision Card only a selection of questions, treatments and information could be included. Also, sufficient evidence was not available to answer the questions properly for all treatment options. Since this might influence the treatment decision, it was mentioned on the Decision Cards whenever applicable. As the surveys for the most important questions were dispersed via a link on the websites of patient societies, response rates cannot be calculated. In both psoriasis and AE research many different outcome measures are used (32–34). Due to this heterogeneity it is difficult to compare evidence. Future studies should preferably report core outcomes (35). To promote high-quality control criteria for PDAs, the International Patient Decision Aids Standards (IPDAS) criteria were developed (36). Unfortunately, these criteria are not yet suitable for EDAs due to their compact size, but it is hoped that they will be applicable in the near future (14). Lastly, since the Dutch treatment guidelines were leading in the development of these Decision Cards, not all available treatments were discussed, and the answers provided on the Decision Cards can differ from other guidelines. Physicians from other countries are advised to check whether these decision cards are suitable for their country. There is a need to update the Decision Cards regularly in the future with the best available evidence. In order to do so, it might be favourable to base Decision Cards on living, international guidelines in the future, and adapt them to the availability of therapies in each specific country. If living, international guidelines do not become available in the near future, the Decision Cards should be updated with every guideline update, as currently agreed.
Future perspective
It is hoped that more Decision Cards will be developed, especially for topical, photo and systemic therapies in psoriasis, and eventually also for the (newer) biologics in both psoriasis and AE. In addition, the impact of Decision Cards on SDM in clinical practice should be evaluated. It might be helpful to develop EDAs that present information more graphically rather than textually.
To fully benefit from decision aids it is important that they are properly implemented. This will require a change in clinical routine and more attention for SDM during a consultation (5). Although some physicians feel SDM takes up too much time, SDM might also save time in the long run, through better compliance, better outcomes and selecting the correct treatment the first time a treatment-decision needs to be made (8). Decision Cards should not replace the conversation between the patient and physician, and physicians should provide patients with extra information if the decision card is not entirely suitable to their personal situation. Furthermore, in order to properly inform patients and enhance SDM correctly, the quality of decision aids is of importance. There is therefore a need to harmonize the development of decision aids, including EDAs. For this reason, we have started a collaboration with multiple other dermatology departments in the Netherlands, in order to reduce duplication of effort and resource expenditure, and we encourage others to do the same.
The authors would like to thank all participating patients, Sanne Snoeijs and Hester Eggink for their contributions to the Decision Cards.
This project was initiated by the Dutch Association of Medical Specialists and the Netherlands Patient Federation., The project was funded by the Quality Funds Foundation of the Dutch Association of Medical Specialists, and was part of a larger initiative to create Decision Cards for common diseases in various medical fields.
Conflicts of interest: GK was involved as sub-investigator in clinical trials for Abbvie, Novartis, LeoPharma, Lilly, Janssen and Regeneron. PS has served as a consultant to AbbVie, Anacor, Leo Pharma, Novartis and Sanofi, has received independent research grants from Leo Pharma and Schering-Plough (> 5 years ago), has been involved in performing clinical trials with many pharmaceutical industries that manufacture drugs used for the treatment of psoriasis and atopic eczema, and is Chief Investigator of the Dutch AE registry – TREAT NL. RT was a consultant to Novartis, Sanofi and Janssen, and has received an independent research grant from Novartis. MV was involved as sub-investigator in clinical trials for Abbvie, LeoPharma, Lilly, Janssen and Regeneron.


 Click to show fullsize
Click to show fullsize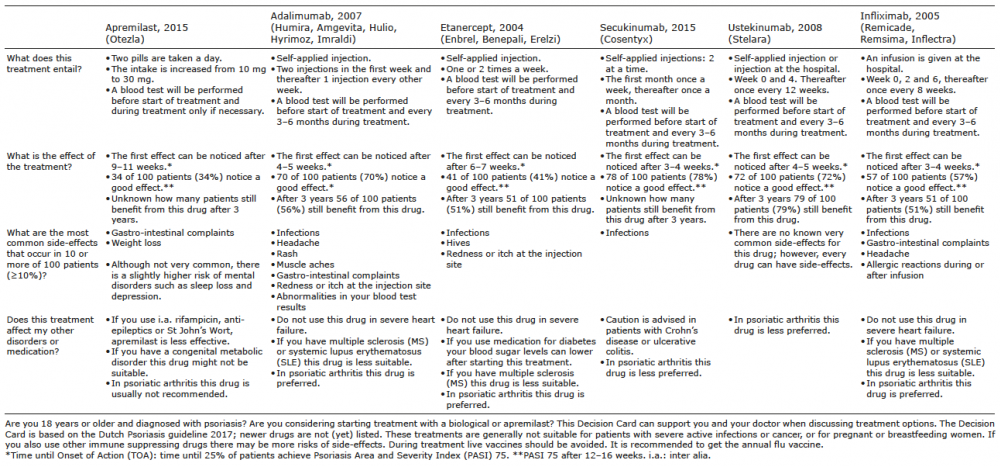 Click to show fullsize
Click to show fullsize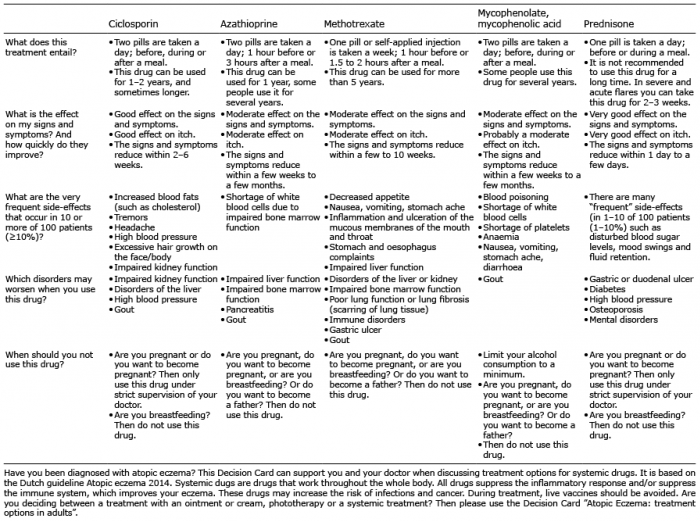 Click to show fullsize
Click to show fullsize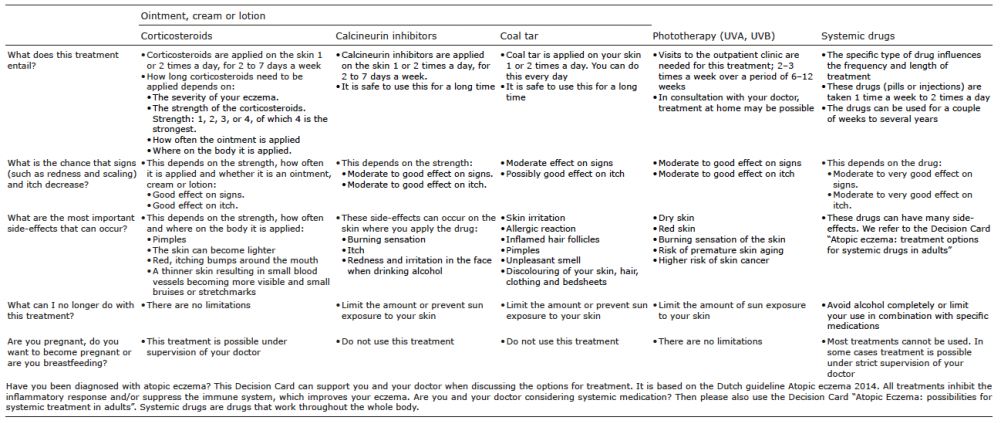 Click to show fullsize
Click to show fullsize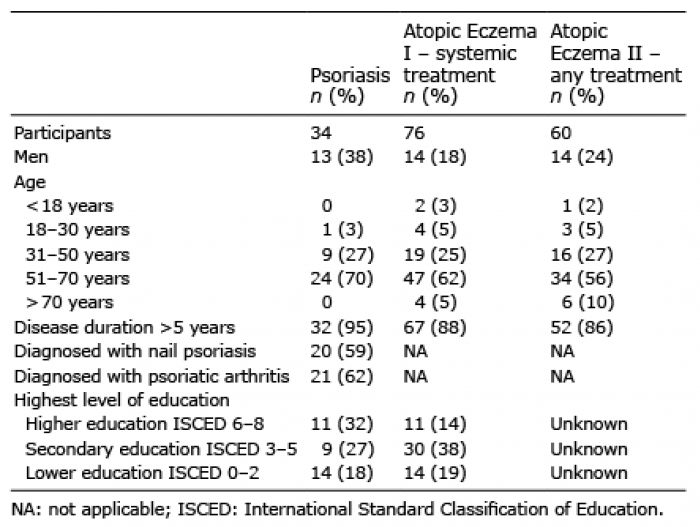 Click to show fullsize
Click to show fullsize