


1Department of Dermatology, Hospital de la Santa Creu i Sant Pau, Universitat Autònoma de Barcelona, Barcelona, Catalonia, Spain, 2DermEdge Research and Probity Medical Research, Mississauga, Ontario, Canada, 3Eli Lilly and Company, Indianapolis, IN, USA, 4HaaPACS GmbH, Schriesheim, Germany (formerly), and 5Radboud University Nijmegen Medical Centre, Nijmegen, The Netherlands
Patient-reported outcomes are valuable for assessing new psoriasis therapies. This study investigated patient-reported outcomes in patients with moderate-to-severe plaque psoriasis treated with ixekizumab or ustekinumab, dosed according to their respective labels, for 52 weeks (IXORA-S-NCT02561806). Patient- reported outcomes investigated included patient global assessment, pruritus, skin pain, health-related quality of life, and work productivity. Ixekizumab-treated patients reported greater improvements in patient- reported outcomes sooner after treatment compared with ustekinumab-treated patients, and maintained greater improvements in patient global assessment scores (ixekizumab 0.72, ustekinumab 1.19; p < 0.001), rates of Dermatology Life Quality Index (0, 1) (ixekizumab 71.3%, ustekinumab 56.6%, p < 0.01), and 36-item Short-form Health survey physical component summary score change from baseline (ixekizumab 5.53, ustekinumab 3.28; p < 0.05) at week 52. While clinically meaningful improvements in patient-reported outcomes resulted with either treatment, ixekizumab provided more rapid improvements in patient-reported outcomes and superior outcomes for some assessments through one year of treatment, while maintaining statistically superior improvements in skin severity, as assessed by either physicians or patients.
Key words: patient-reported outcomes; health-related quality of life; ixekizumab; ustekinumab.
Accepted Nov 16, 2020; Epub ahead of print Nov 25, 2020
Acta Derm Venereol 2020; 100: adv00344.
doi: 10.2340/00015555-3700
Corr: Lluís Puig, Department of Dermatology, Hospital de la Santa Creu i Sant Pau, Universitat Autònoma de Barcelona Medical School, Mas Casanovas 90, ES-08041 Barcelona, Spain. E-mail: lpuig@santpau.cat
While skin clearance is the goal of psoriasis treatment, patients and practitioners also state the need for improvements in patients’ quality of life. These improvements are evaluated by various patient-reported outcomes. The results of this study showed that ixekizumab-treated patients had significantly greater improvements in patient-reported outcomes compared with ustekinumab-treated patients across multiple assessments at or before week 12, with the responses being maintained to week 52. As most patients in the IXORA-S trial achieved high levels of skin clearance, the trial results presented here reflect the important improvements in everyday quality of life that come with skin clearance.
Resolution of skin plaques is the key endpoint for any psoriasis trial; however, patients and physicians also state the need for equal improvements in patients’ quality of life, as measured by patient-reported outcomes (PROs) (1–3). Because psoriasis affects patients both physically and psychologically (4–9), for new therapeutics it is valuable to examine PROs in the context of skin clearance.
IXORA-S was a phase 3, head-to-head trial comparing ixekizumab, a high-affinity monoclonal antibody that selectively targets interleukin (IL)-17A (10), with ustekinumab, an antibody that targets IL-12/23 (11). At week 12 primary endpoint, and continuing through to week 52, ixekizumab was found to be more effective than ustekinumab, as assessed by Psoriasis Area and Severity Index (PASI) 75/90/100 and the static Physician’s Global Assessment (sPGA) (0, 1) response rates, and safety outcomes were comparable (12, 13). Improvements in PROs, including Itch Numeric Rating Scale (NRS) minimal clinically important difference rates and Dermatology Life Quality Index (DLQI) scores of (0, 1), were also statistically significantly greater for ixekizumab-treated patients compared with ustekinumab-treated patients as early as weeks 2 and 24 (12). The aim of the current study was to assess whether ixekizumab treatment lead to greater and more rapid improvements in PROs, compared with ustekinumab treatment, through to week 52 of IXORA-S.
Study design
IXORA-S (NCT02561806) was a phase 3b, multicentre, randomized, double-blinded, double-dummy, active comparator, and parallel-group trial (12, 13). Patients were randomized 1:1 to receive ixekizumab (IXE; 160 mg starting dose, 80 mg every 2 weeks through to week 12, 80 mg every 4 weeks through to week 52) or ustekinumab (UST; dosed per label, patients ≤ 100.0 kg received 45 mg and patients > 100.0 kg received 90 mg at weeks 0 and 4, then every 12 weeks through to week 52). This study reports the outcomes from baseline to week 52 using validated tools to assess clinical disease severity and patient-reported outcomes (PROs). Some PROs were previously reported for weeks 0–24 (12). The primary endpoint of the study was to assess the proportion of patients achieving a PASI 90 response at week 12 (12).
Study population
Key inclusion and exclusion criteria have been reported previously (12). Of note, eligible study participants were required to have a baseline PASI ≥ 10; to have previously failed, had a contraindication, or exhibited an intolerance to at least one systemic therapy; and no prior treatment with ustekinumab, ixekizumab, or any other interleukin (IL)-17 or IL-12/23 antagonists.
Ethical compliance
Study protocols were approved by applicable Ethical Review Boards (ERB) (study number NCT02561806). The study was performed in accordance with the Council for International Organizations of Medical Sciences International Ethical Guidelines and the principles of the Declaration of Helsinki.
Outcome measures
Psoriasis Area and Severity Index (PASI). PASI scores range from 0 (no psoriasis) to 72 (most severe disease).
Static Physician’s Global Assessment. Physician’s assessment rated on a 6-point scale (0: clear; 1: minimal; 2: mild; 3: moderate; 4: severe; 5: very severe).
Patient Global Assessments (PtGA). Patient-administered, scale rated on a 0 (clear) to 5 (severe) numerical rating scale (NRS).
Itch numerical rating scale (NRS). A validated patient-reported NRS assessing itch severity on a 0 (no itch) to 10 (worst itch imaginable) scale (14). A minimal clinically important difference (MCID) is an improvement ≥ 4 among patients who reported an Itch NRS score ≥ 4 at baseline (15).
Skin pain visual analogue scale (VAS). A patient-reported tool assessing current skin pain on a 0-mm (no pain) to 100-mm (severe skin pain) horizontal scale.
Dermatology Life Quality Index (DLQI). A validated patient-administered questionnaire with 10 questions spanning 6 domains (symptoms and feelings; daily activities; leisure; work and school; personal relationships; and treatment) with a total score ranging from 0 to 30 (16, 17); scores of 0 or 1 (0, 1) represent no impact of disease on health-related quality of life (HRQoL) (18).
Medical outcomes study 36-item Short-Form health survey (SF-36). SF-36 assesses 8 domains: physical functioning, role-physical, role-emotional, bodily pain, vitality, social functioning, mental health, and general health (19, 20). Composite physical health (PCS) and mental health (MCS) component scores were derived from the individual domains. Lower scores denote greater impairments in quality of life. The acute (one-week recall) version of the scale was used.
European Quality of Life – 5 Dimensions – 5 Level (EQ-5D-5L) and European Quality of Life for Psoriasis (EQ-PsO). The EQ-5D-5L measures dimensions of mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Scores were converted into a single summary index by crosswalking the data using UK population-based index scores (21). The EQ-PsO adds 2 additional psoriatic disease-specific dimensions (skin irritation (itching) and self-confidence) to the standard EQ-5D-5L questionnaire (22). In addition, the 100-mm VAS was used for patient reporting of current health state, with 100-mm indicating “best imaginable health state” and 0-mm indicating “worst imaginable health state”.
Work Productivity and Activity Impairment Questionnaire for Psoriasis (WPAI:PsO). The WPAI:PsO evaluates 4 dimensions: absenteeism, presenteeism, work productivity loss, and activity impairment (23). Higher scores indicate greater impairment.
Statistical analysis
For continuous variables, mean and standard deviation (SD) are reported; for binary variables both absolute and relative frequencies are reported. Continuous variables were compared using the Wilcoxon rank sum test. Missing values for continuous variables were imputed using modified baseline observation carried forward (mBOCF) (24). Binary variables were compared using Fisher’s exact test. Missing values for binary variables were imputed using non-responder imputation. All statistical tests were 2-sided. p-value < 0.05 were considered statistically significant. No multiplicity adjustments were performed for these analyses. All analyses were performed using SAS Version 9.4 (Cary, NC: SAS Institute Inc; 2014.) and were pre-specified except for the analysis of Itch NRS score distribution over time.
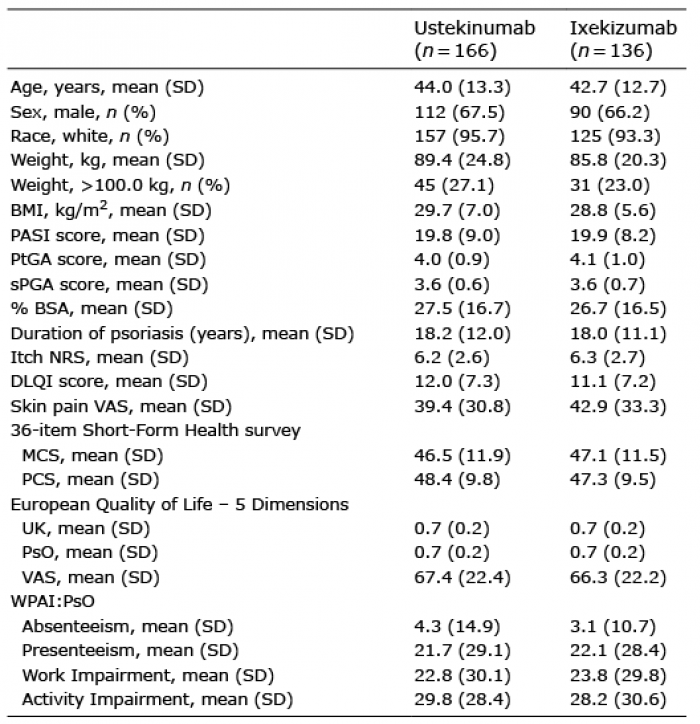
Baseline demographics and patient characteristics were well balanced between the ixekizumab (n = 136) and ustekinumab (n = 166) treatment arms (Table I). Baseline PASI, PtGA, and sPGA were indicative of moderate-to-severe disease activity. Baseline itch NRS and skin pain VAS scores were also moderate in severity. Baseline DLQI total scores were aligned with moderate-to-severe disease (DLQI>10) (25). SF-36 MCS and PCS indicated a moderate impact on patient HRQoL.
Table I. Baseline patient demographics and clinical characteristics
Both patient and physician assessments of disease severity were investigated using evaluation of sPGA (Fig. 1A) and PtGA (Fig. 1B), respectively, over a period of 52 weeks. Patients in both treatment groups demonstrated rapid improvements in PtGA and sPGA scores (as assessed by change from baseline) during the first 12 weeks, which continued through to week 52 for PtGA (IXE 0.72 ± 0.94 (mean ± SD), UST 1.19 ± 1.21) and sPGA (IXE 0.64 ± 0.92, UST 1.14 ± 1.20). PtGA and sPGA scores in the ixekizumab treatment group were statistically significantly more improved, compared with the ustekinumab treatment group, at all post-baseline assessments. Of note, both sPGA and PtGA scores within treatments exhibited numerically similar trends, indicating that patient and physician disease perspectives were similar for these assessments.
Fig. 1. Static Physician’s Global Assessment (sPGA) and patient global assessments (PtGA) among patients with psoriasis treated with ixekizumab (IXE) or ustekinumab (UST) for 52 weeks. PtGA: ?p < 0.01, ‡p < 0.001 UST vs IXE; sPGA: **p < 0.01, ***p < 0.001 UST vs IXE. p-values derived from Wilcoxon rank sum test. mBOCF: modified baseline-observation carried forward.
Pruritus is one of the leading symptoms in patients with chronic plaque psoriasis. Patients treated with ixekizumab reported greater improvements in Itch NRS sooner after treatment compared with ustekinumab (12), but by week 52, improvements in itch severity were not different between treatment groups (Fig. 2A; IXE–5.01 ± 2.96, UST –4.55 ± 2.85). A similar trend was seen for the proportion of patients achieving Itch NRS MCID (improvement ≥ 4, Fig. 2B). A statistically significantly greater proportion of ixekizumab-treated patients achieved Itch NRS (0) early in treatment compared with ustekinumab-treated patients (Fig. 2C), but by week 52, similar proportions of patients in each treatment group reported complete resolution of their itch symptoms (IXE 41.2%, n = 56, UST 34.3%, n = 57).
Fig. 2. (A) Change in Itch numerical rating scale (NRS) scores, and (B) the proportions of patients achieving Itch NRS minimal clinically important difference (MCID) (≥ 4 improvement) or (C) Itch NRS (0) when treated with ixekizumab or ustekinumab for 52 weeks. Achievement of Itch NRS MCID was investigated in patients who had Itch NRS scores ≥ 4 at baseline. Itch NRS scores and proportion of patients achieving Itch NRS MCID previously reported for weeks 0–24 (12) *p < 0.05, **p < 0.01, ***p < 0.001, all vs UST by (A) Wilcoxon rank sum or (B & C) Fisher’s exact test. mBOCF: modified baseline-observation carried forward; NRI: non-responder imputation.
To further investigate the severity of pruritus that had not resolved, individual itch NRS response rate levels were defined and overlaid (Fig. 3). Itch NRS scores ≤ 2 and ≤ 1 (including 0) were reported by similar numbers of ixekizumab-treated and ustekinumab-treated patients at week 12 (≤ 2: IXE n = 99, 72.8%, UST n = 119, 71.7%; ≤ 1: IXE n = 83, 61.0%, UST n = 97, 58.4%). The percentages for Itch NRS scores reported at week 12 for both treatment groups increased slightly, but with some fluctuation, throughout the maintenance period. At week 52, 76.5% (n = 104) of ixekizumab-treated patients and 70.5% (n = 117) of ustekinumab-treated patients rated their pruritus ≤ 2, and 64.0% (n = 87) of ixekizumab-treated patients and 61.4% (n = 102) of ustekinumab-treated patients rated their pruritus ≤ 1. In summary, pruritus reductions were observed earlier in patients treated with ixekizumab, although by week 24, similar responses were seen in both treatment groups and maintained until week 52.
Fig. 3. Response rates for individual Itch numerical rating scale (NRS) scores for (A) ixekizumab-treated and (B) ustekinumab-treated patients through to week 52. Coloured areas: itch NRS responses. Solid vertical line: end of induction period (primary endpoint). Dotted vertical lines: active injections administered during the maintenance period. All patient visits during the maintenance period are represented on the x-axis. Due to missing data at some time-points, total response rates do not always add up to 100, as indicated by the white space at the top of each area plot.
Skin pain improved rapidly from baseline in both treatment groups (12) and persisted throughout the maintenance period (Fig. 4A). At week 52, the mean change from baseline in skin pain VAS score was –36.54 for ixekizumab-treated patients and –31.79 for ustekinumab- treated patients. Complete resolution of skin pain was achieved by 48.5% (n = 66) of ixekizumab-treated patients and 41.0% (n = 68) of ustekinumab-treated patients at week 52 (Fig. 4B).
Fig. 4. Change in (A) skin pain visual analogue scale (VAS) and (B) the proportions of patients achieving Skin Pain VAS (0) when treated with ixekizumab (IXE) or ustekinumab (UST) for 52 weeks. *p < 0.05, **p < 0.01, ***p < 0.001, all vs UST by (A) Wilcoxon rank sum or (B) Fisher’s exact test. Skin pain VAS scores previously reported for weeks 0–24 (12). mBOCF: modified baseline observation carried forward; NRI: non-responder imputation.
Improvements in HRQoL, as assessed by DLQI, were statistically significantly greater for ixekizumab-treated patients within the first month of treatment (week 2 IXE: –6.34, UST: –3.55; week 4 IXE: –7.79, UST: –5.72; Fig. 5A); however, DLQI change from baseline scores were similar at assessed time-points thereafter. DLQI (0, 1) rates were statistically significantly greater in the ixekizumab treatment group, at all post-baseline assessments (Fig. 5B). At week 52, 71.3% (n = 97) of ixekizumab-treated patients and 56.6% (n = 94) of ustekinumab-treated patients reported minimal-to-no impact of their disease (DLQI [0, 1]). DLQI component scores are shown in Table SI.
Fig. 5. Change in (A) Dermatology Life Quality Index (DLQI) total scores and (B) the proportion of patients achieving DLQI (0, 1) for patients with psoriasis treated with ixekizumab (IXE) or ustekinumab (UST) for 52 weeks. DLQI (0, 1) results previously reported for weeks 0–24 (12). **p < 0.01, ***p < 0.001, both vs UST by Wilcoxon rank sum test. mBOCF: modified baseline-observation carried forward; NRI: non-responder imputation.
HRQoL was also investigated using SF-36 and EQ-5D. Patients treated with ixekizumab reported statistically significantly greater improvements in SF-36 PCS change from baseline at all post-baseline assessments, including week 52 (IXE: 5.53, UST: 3.28; Fig. 6A). No statistical differences were seen between treatment groups in SF-36 MCS change from baseline (Fig. 6B). Individual SF-36 domains are shown in Table SII.
Fig. 6. Change in 36-item Short-Form Health survey (SF-36) (A) physical and (B) mental component summaries for patients with psoriasis treated with ixekizumab (IXE) or ustekinumab (UST) for 52 weeks. *p < 0.05 vs UST by Wilcoxon rank sum test. mBOCF: modified baseline-observation carried forward.
Improvements in EQ-5D-5L index score, EQ-PsO index score, and EQ-5D VAS were observed in both treatment groups (Table II). While statistically significantly greater improvements in the EQ-PsO Index Score were reported for ixekizumab-treated patients at weeks 12 (IXE: 0.1512, UST: 0.1173) and 24 (IXE: 0.1561, UST: 0.1210), all other EQ-5D results were comparable between the 2 treatment groups.
Table II. Changes in quality of life outcomes reported by patients with psoriasis treated with ixekizumab (IXE) or ustekinumab (UST) for 52 weeks
Finally, rapid improvements in work productivity and activity impairment, as assessed by the WPAI:PsO questionnaire, were observed in both treatment groups (Fig. 7) with no statistical differences observed in any WPAI:PsO domains between the 2 treatment groups.
Fig. 7. Change in the domains of the Work Productivity and Activity Impairment Questionnaire for Psoriasis (WPAI:PsO) Impairment for patients with psoriasis treated with ixekizumab (IXE) or ustekinumab (UST) for 52 weeks including (A) Absenteeism, (B) Presenteeism, (C) Work Productivity Loss, and (D) Activity Impairment. mBOCF: modified baseline-observation carried forward.
Overall, in these analyses, treatment with ixekizumab resulted in greater improvements in PROs, compared with ustekinumab treatment, early in treatment. However, both treatments resulted in important clinical improvements in PROs for patients, which were maintained through to week 52. In patients treated with ixekizumab, improvements in disease activity (sPGA and PtGA) and HRQoL remained statistically significantly superior, vs ustekinumab, throughout the maintenance period (including week 52).
It is not uncommon for discordances to be observed between physician and patient-reported outcomes (26, 27). Disease severity assessments in this study allowed for an observational comparison of patient-reported and physician-reported subjective measures. Overlap (within treatment groups) between sPGA and PtGA scores throughout the study indicate similarities between physician and patient perception of disease severity. While other studies have indicated discordant scoring between patient and physician scales (26, 27), IXORA-S has provided an example of alignment between the 2 scales.
High physician-reported disease severity is associated with a greater severity of patient-reported symptoms (pruritus, pain), HRQoL, and impact on work productivity (9). Furthermore, improvements in clinical responses are associated with improvements in PROs (28, 29). As published previously, 52.2% and 76.5% patients treated with ixekizumab achieved PASI100 (completely clear skin) and PASI90 by week 52, respectively, vs 35.5% and 59.0%, respectively, of patients treated with ustekinumab (13). PRO results presented here illustrate greater improvements in ixekizumab-treated patients, particularly early in treatment, compared with ustekinumab-treated patients. Given that the majority of patients treated in IXORA-S achieved PASI90 or PASI100, it follows that these patients would report clinically significant improvements in a number of PROs, as reflected in the results of the current study.
Study limitations and strength
Limitations of this study include lack of a placebo arm, potentially biasing PROs, and the relatively short trial duration. Changes in quality of life may require longer treatment periods in order for the benefits of treatment to peak, as opposed to outcomes assessing itch or pain. In addition, these medications possess differences in their peak onset of efficacy, as previously noted (12); therefore, the timing of peak improvements in PROs and their association with peaks in clinical efficacy may differ between the 2 treatments.
A strength of this analysis is the inclusion of disease-specific validated PRO measures to highlight the patient perspective in psoriasis.
Conclusion
Ixekizumab treatment resulted in greater improvements at or before week 12 across the majority of PRO measures, compared with ustekinumab treatment; both treatments resulted in clinically meaningful improvements for patients across the PROs assessed, and these responses were maintained through to 52 weeks (12).
Brian S. Comer, PhD, and Chenyun Tan, PharmD, for medical writing assistance during the preparation of this manuscript. Kannan R MSc, MTech for editorial assistance during the preparation of this manuscript. Russel Burge for his advice on PRO measures.
Conflicts of interest: LP reports receipt of honoraria or consultation fees from Abbvie, Almirall, Amgen, Baxalta, Biogen, Boehringer Ingelheim, Celgene, Gebro, Janssen, Leo Pharma, Lilly, Merck Serono, MSD, Mylan, Novartis, Pfizer, Regeneron, Roche, Sandoz, Samsung-Bioepis, Sanofi, and UCB. ML reports receipt honoraria and/or consultation fees from Abbvie, Amgen, Bristol Myers Squibb, Boehringer Ingelheim, Dermira, Janssen, Leo Pharma, Lilly, Merck Serono, Novartis, Pfizer, Regeneron, Sandoz, Sun Pharma, Sanofi, and UCB. KH and YD are employees and shareholders of Eli Lilly and Company. LB was a former employee of HaaPACS GmbH on behalf of Eli Lilly and Company. PvdK reports fees for consultancy service or lectureships from Celgene, Almirall, Abbvie, Amgen, Eli Lilly, Novartis, Janssen Pharmaceutica, Leo Pharma, Bristol Myers Squibb and Dermavant.


 Click to show fullsize
Click to show fullsize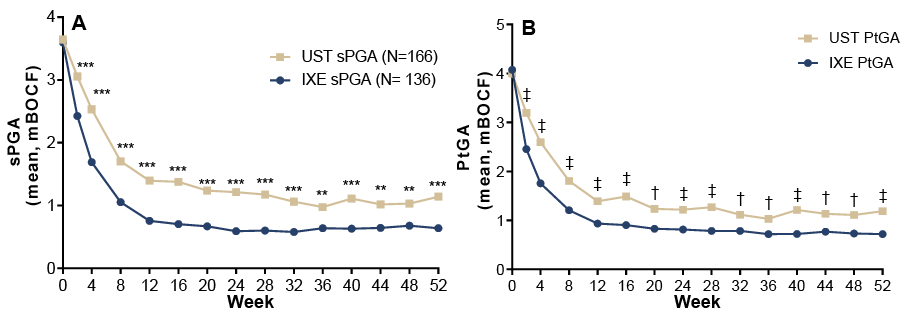 Click to show fullsize
Click to show fullsize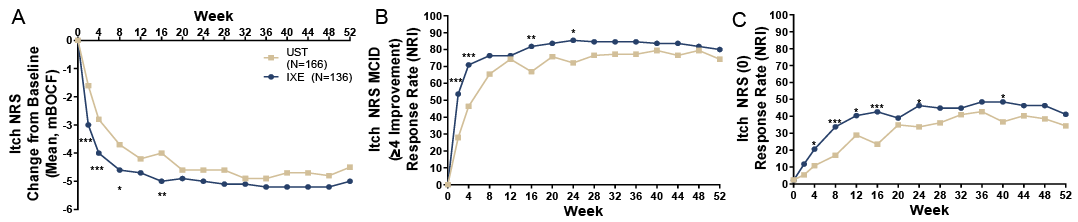 Click to show fullsize
Click to show fullsize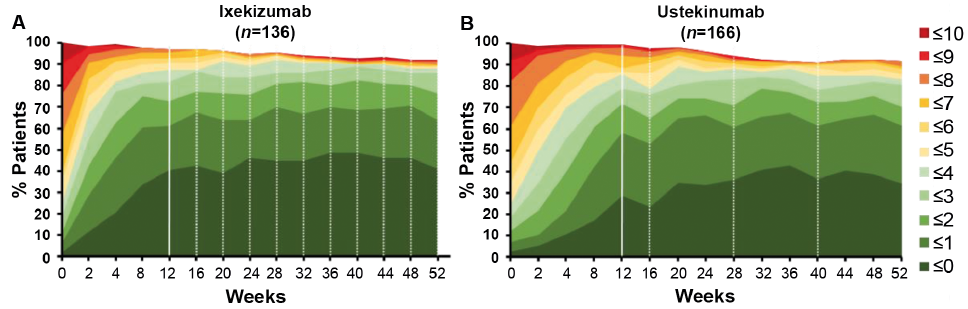 Click to show fullsize
Click to show fullsize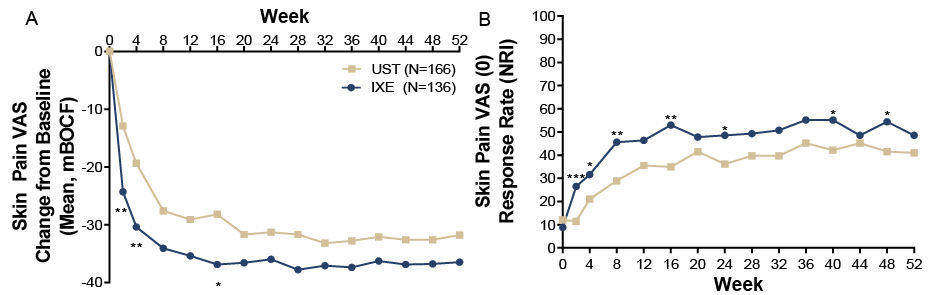 Click to show fullsize
Click to show fullsize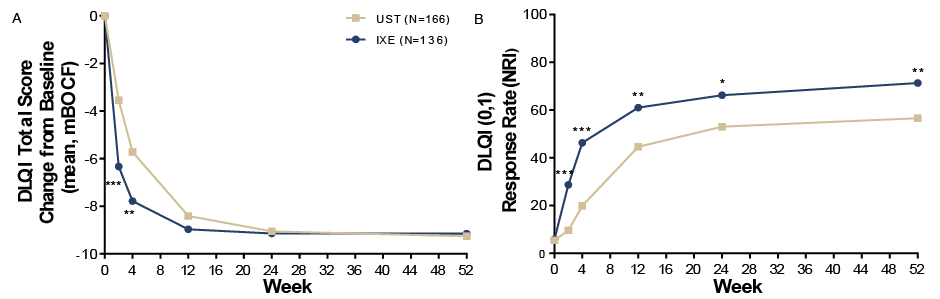 Click to show fullsize
Click to show fullsize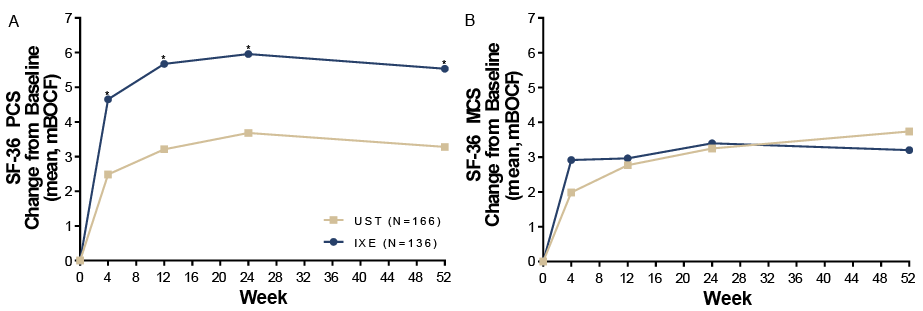 Click to show fullsize
Click to show fullsize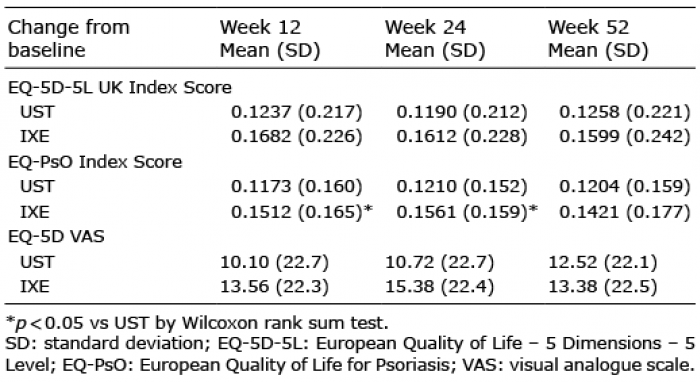 Click to show fullsize
Click to show fullsize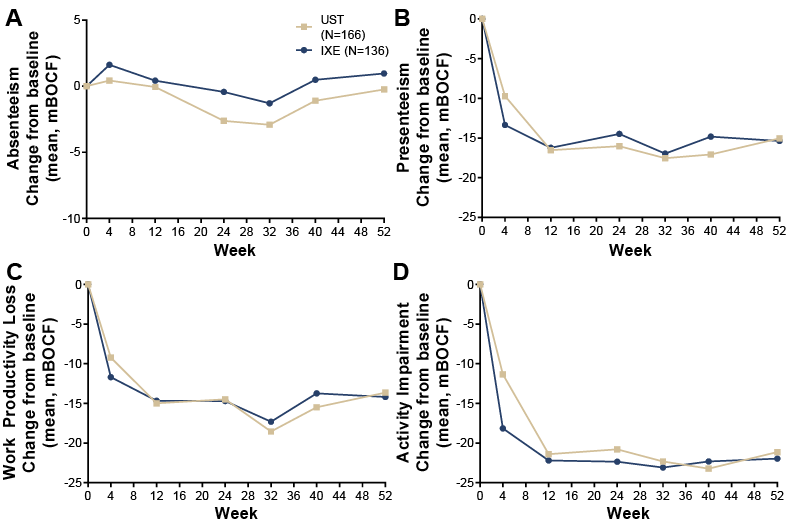 Click to show fullsize
Click to show fullsize