


1Department of Dermatology and Allergology, Skin and Allergy Hospital, Helsinki University Hospital, and 2University of Helsinki, Helsinki, Finland
Previous research presents pulsed dye laser-mediated photodynamic therapy as a promising alternative to conventional red-light photodynamic therapy. In this study, 60 patients with 2 or more actinic keratoses randomly received either of these treatments on each side of the head. A physician blinded to the treatment evaluated treatment response at 6 months for each lesion, as completely, partially or not healed. Significantly lower complete clearance rates (10.3% vs 44.9%) and lesion-specific complete clearance rates were found for pulsed dye laser-mediated photodynamic therapy (47.9%) vs conventional red-light photodynamic therapy (73.4%). Significantly lower pain scores were found for pulsed dye laser-mediated photodynamic therapy, with a mean numerical rating of 2.3, compared with 4.1 for conventional red-light photodynamic therapy. The study population had a mean of 7.9 lesions, and 78% of patients had been treated previously for actinic keratoses on the treatment area. To conclude, in a population with severe sun damage, pulsed dye laser-mediated photodynamic therapy seems less effective than conventional red-light photodynamic therapy. Pulsed dye laser-mediated photodynamic therapy may still be a treatment option for patients who are not compliant with conventional red-light photodynamic therapy.
Key words: actinic keratosis; photochemotherapy; lasers; dye.
Accepted Jan 21, 2021; Epub ahead of print Jan 25, 2021
Acta Derm Venereol 2021; 101: adv00404.
doi: 10.2340/00015555-3754
Corr: Vivian Lindholm, Department of Dermatology and Allergology, Skin and Allergy Hospital, Helsinki University Hospital, Meilahdentie 2, FIN-00250, Helsinki, Finland. E-mail: vivian.lindholm@helsinki.fi
Actinic keratoses, which are common precancerous lesions of the skin, arise from chronic lifetime sun exposure. A useful treatment method is photodynamic therapy (PDT), but this can cause strong pain during treatment. This study compared PDT using an alternative illumination source, pulsed dye laser, with conventional PDT in 60 patients with multiple actinic keratoses, in a randomized split-face design. Laser treatment was significantly less painful; however, in contrast to previous research, it was less effective than conventional PDT, with a complete clearance rate of 10% at 6 months in the laser treatment group compared with 45% in the conventional treatment group.
Actinic keratoses (AKs) are common premalignant lesions of the skin that have a risk of developing into invasive squamous cell carcinoma (SCC) (1, 2). AK favour sun-exposed areas, such as the head, as chronic sun exposure increases their risk as well as high age, fair skin and immunosuppressive medication (3). Photodynamic therapy (PDT) is considered a first-line treatment for patients with multiple AKs (4). In PDT, a light-sensitizer containing a substrate of protoporphyrin IX (PpIX) is applied to the skin. PpIX then accumulates in transformed cells more than in the surrounding healthy cells, and the subsequent illumination causes an oxygen radical reaction in the tumour cells, which destroys the cells (5). Previous studies have found the treatment response of PDT to be excellent, with clearance achieved in 89–92% of cases (6, 7). However, PDT can cause strong pain during treatment and is laborious both for the patient and the hospital, introducing a need for less painful and less time-consuming treatment options. Previously, 585-nm pulsed laser-mediated PDT (PDL-PDT) was introduced as an alternative light source for PDT because of a peak in the light absorption of PpIX in the 585-nm light range (8). Previous studies suggest that PDL-PDT serves as a nearly or equally as effective and less painful treatment option than conventional PDT (cPDT), but the evidence is scarce. To our knowledge, there are 4 published studies, which are mostly limited by a short follow-up, small sample size, non-blinded or non-randomized designs (8–11).
This 6-month prospective study at the Helsinki University Hospital (HUS) Skin and Allergy Hospital in 2018 to 2020 included 60 patients with at least 2 AKs distributed symmetrically on both sides of either the scalp, forehead or cheeks. Using simple randomization, patients randomly received PDL-PDT treatment for all the lesions on half of the head and cPDT as control treatment on all lesions on the other half. For patients with extensive field cancerization, the treatment field was split into 2 parts, treated with either PDL-PDT or cPDT. Study patients were recruited from patients who were seen for follow-ups at the clinic due to recurrent skin tumours or premalignancies, or from patients referred to the clinic because of multiple AKs on the head. The study included patients over 18 years of age with Fitzpatrick skin types I to III (12). Exclusion criteria were: suspicion of pigmented AK, in-situ carcinomas, skin cancers, psoriasis or seborrhoeic eczema on the treatment area. Patients were invited to a 6-month follow-up appointment. For 15 patients, the follow-up was postponed to 9 months because of the COVID-19 epidemic. One patient was not able to attend the 6-month follow-up, and one was excluded early from the analyses because they were given the wrong treatment parameters. Thus, the final analyses included 58 patients.
At the first appointment, the treatment area was photographed, a physician numbered the lesions, marked them on a plastic sheet to specify their location, and graded their severity on the Olsen scale, from I to III (13). After curettage and haemostasis with aluminium chloride, a light-sensitizer (methyl aminolaevulinate cream, Metvix®, Galderma, La Tour-de-Peilz, Switzerland) was applied in a layer 1-mm thick on the lesions and covered with an occlusive plastic foil for 2–3-h incubation. Before treatment, a local lidocaine anaesthetic spray was applied. The PDL-PDT-–treated lesions were illuminated with 30% overlapping pulsed laser double-stacked pulses (Candela Vbeam perfecta® (Wayland, MA, USA), energy 7 J/cm2, spot size 7 mm, pulse duration 10 ms, wavelength 595 nm and dynamic cooling 2/3) and the cPDT-treated lesions with a red LED light for 7–8 min (Actilite® CL 128 (Galderma), exposure 75 J/cm2, wavelength 630 nm). The side of the head not being treated was covered with aluminium foil during illumination. All patients were asked to evaluate the maximal pain during both illuminations on a 1–10 numerical rating scale (NRS). If needed, additional injection (n = 1) or regional (n = 1) nerve block anaesthesia with lidocaine was used. These patients were excluded from the pain analyses.
At the follow-up appointment, a blinded investigator evaluated the treatment results for each treated lesion. For lesions that did not heal, the physician planned their further care. Only persistent lesions were documented, but not new untreated ones outside the treatment field. All the recruited volunteer patients were informed of the evaluations orally and in writing, and provided written consent. The study protocol was approved by the HUS ethics review committee.
Statistical methods
The results are presented as patient complete clearance rates (CC), defined as all treated lesions of the patient in the corresponding treatment completely healed; and partial clearance rates (PC), defined as 75% of lesions of the patient in the treatment completely healed. In addition, the lesion-specific clearance rates (LSC), referring to the proportion of individual lesions that were completely, partially or not healed in both treatments, are presented. Cross-tabulation combined with McNemar’s test was used for the CC and PC analyses and Pearson’s χ2 and Cochran–Armitage trend tests for the LSC analyses. Confounding factors were determined using Student’s t-test and Mann–Whitney U test. For the pain calculations, the paired t-test was used. The analyses were performed using NCSS statistical software 12.09 (NCSS, Kaysville, UT, USA). Significance was set at p < 0.05.
Baseline characteristics
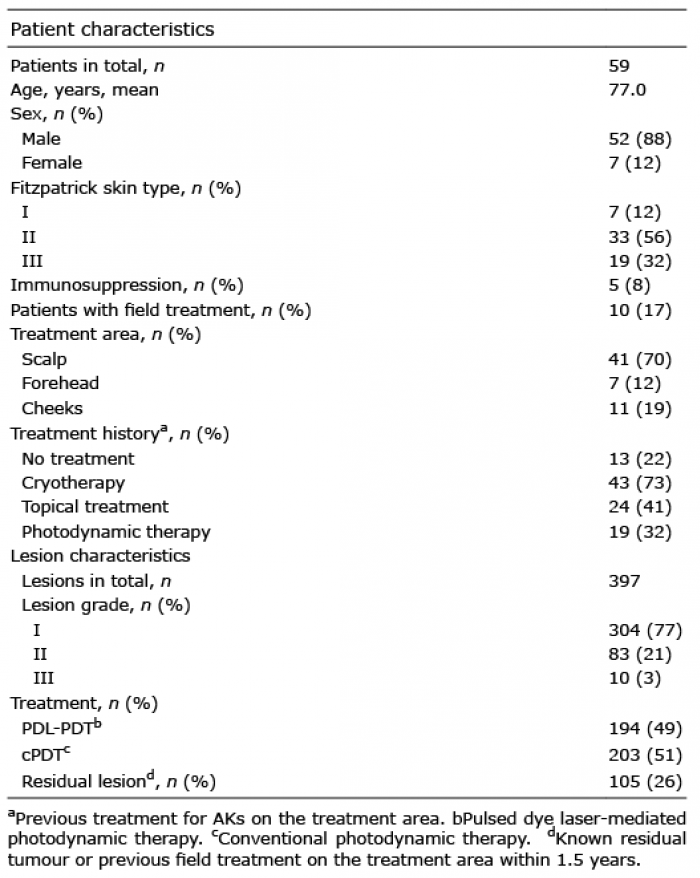
The mean age of the study population was 77.0 years; there were 7 women and 52 men. Five had immunosuppressive medication, one had azathioprine and one methotrexate combined with prednisolone, 2 prednisolone alone and one abiraterone acetate. None of the patients was an organ transplantation patient. The scalp was the most common treatment area (70%). The study population had either a mean of 7.9 individual lesions (mean 3.4 PDL-PDT-treated lesions and 3.5 cPDT-treated lesions) or one large field treatment area, without separate individual lesions (n = 10, 17%). A total of 25 patients had PDL-PDT treatment on all lesions on the left side of the head and 34 patients on the right side of the head. A total of 397 lesions were treated; 194 lesions with PDL-PDT and 203 with cPDT. One field treatment area is counted here as 1 AK. Thirteen patients had no previous treatment for AKs on the treatment area (Table I).
Table I. Baseline characteristics
Complete and partial clearance rates
A statistically significant difference (p < 0.00) was observed in the treatment response, with complete clearance achieved in 10.3% of patients with PDL-PDT treatment and 44.9% with cPDT (Table I). Regarding partial clearance, the corresponding values were 29.3% in PDL-PDT and 60.3% in cPDT (p < 0.00) (Fig. 1).
Fig. 1. Complete and partial (75%) clearance rates (n (%)) in pulsed dye laser-mediated photodynamic therapy (PDL-PDT) and conventional photodynamic therapy (cPDT) differed significantly (p < 0.00).
Lesion-specific clearance rates
The lesion-specific clearance rates for both treatments differed significantly (p < 0.00, Fig. 2). In PDL-PDT, 47.9% of the lesions healed completely and 32.5% healed partially; correspondingly for cPDT, 73.4% healed completely and 21.7% healed partially. Thus, 19.6% of PDL-PDT-treated lesions and 4.9% cPDT-treated lesions did not heal (Fig. 2). No significant confounding factors were observed when adjusting for age, sex, skin type, lesion grade, residuals, previous treatment on the area, treatment area and immunosuppression (p > 0.9). No SCCs or in situ carcinomas arose on the treatment area during the 6-month follow-up.
Fig. 2. Lesion-specific clearance rates (n (%)) in pulsed dye laser-mediated photodynamic therapy (PDL-PDT) and conventional photodynamic therapy (cPDT) with a significant difference (p < 0.00).
Secondary outcomes
A significantly lower treatment response was found in PDL-PDT for thin lesions (grade I, n = 304). However, for thick lesions (grades II–III, n = 93), no significant difference was observed (p = 0.26) with 50.0% of the lesions healed in PDL-PDT vs 61.0% in cPDT. A significantly lower treatment response was observed in PDL-PDT compared with cPDT irrespective of the previous treatment history of the area (p < 0.00 if no previous treatment, p = 0.02 if previous cryotherapy, and p < 0.00 if previous field treatment on the area).
Treatment tolerability
A significantly lower pain rate (p < 0.00) was observed in PDL-PDT treatment, with a mean pain score (NRS) of 2.3, and NRS 4.1 in cPDT. The eta coefficient showed a weak correlation between pain and CC (0.28) and a negligible correlation between pain and PC (0.18), implying that pain contributes to 8% of the variance in the complete clearance rates and 3% of the variance in the partial clearance rates (Fig. 3).
Fig. 3. Boxplot of the mean values for patient-reported pain on the numerical rating scale (NRS) in pulsed dye laser-mediated photodynamic therapy (PDL-PDT) and conventional photodynamic therapy (cPDT) (p < 0.00).
Only a few studies have investigated the efficacy of PDL-PDT in the treatment of AKs. Kessel et al. concluded no significant difference comparing PDL-PDT with cPDT in a split-face manner on 57 patients (9). At 6 months, 62% of PDL-PDT-treated and 64% of cPDT-treated AKs had healed, and at 12 months, the corresponding values were 48% and 56%. The study limitations included a non-blinded investigation and a non-randomized study design, and newly developed lesions were not differentiated from persistent ones, as in our study.
Alexiades-Armenakas et al. (10) treated 41 patients with AKs with PDL-PDT. In these patients, 90% of the PDL-PDT-treated lesions had healed at 8 months, 0% in the laser-only control group. Only 10 patients completed the follow-up of 8 months, limiting the reliability of the results. Kim et al. (11) treated 30 patients with PDL-PDT with a limited 3-month follow-up. The lesion complete clearance rates were 67% for PDL-PDT and 73% for cPDT, with a non-significant difference. The lesions were treated up to 5 times at 1–2 weeks apart. Karrer et al. (8) treated 24 patients. The lesion complete clearance rates for both treatments were 79% vs 84%, but the follow-up was limited to one month. At our clinic, a prior licentiate thesis on 51 lesions treated with PDL-PDT and 86 with cPDT, showed complete clearance for 71% of lesions treated with PDL-PDT vs 90% for cPDT at a 6-month follow-up (14). In this study, both treatments were repeated after 2 weeks. In all previous studies, PDL-PDT has a lower clearance rate, but it is mostly statistically insignificant. Our PDL-PDT lesion clearance rates are the weakest, with a clearance rate of 48% at 6 months compared with 62–92% in previous studies. However, in Alexiades-Armenakas et al. (10), the patients’ complete clearance rate for extremity lesions was also low (17% compared with 10% in our study).
Mutually, in all previous studies, PDL-PDT caused significantly less pain during treatment than cPDT. Pain on the visual analogue scale (VAS) in these studies was 1.7–2.6 in PDL-PDT and 4.2–6.5 for cPDT. Our corresponding mean NRS values of 2.3 and 4.1 are in line with the previous results.
For PDL-PDT treatment, the same laser parameters were used as in the study by Kessel et al. (9). The other studies’ parameters were also similar; however, Karrer et al. (8) used a higher 18 J/m2 fluence, Alexiades-Armenakas et al. (10) and Ruohoalho et al. (14) a larger spot size 10 and Kim et al. (11) and Karrer et al. (8) a PDL-PDT wavelength of 585 nm. A weak or negligible association was found between pain values and outcome (CC/PC). An association could suggest that the biological dose achieved in PDL-PDT is lower than in cPDT. However, since PDL-PDT pulses are of a short 10 ms duration compared with 433 s in cPDT, it may not be adequate to evaluate treatment efficacy by the experienced pain. When comparing light doses in both treatments, it is lower in PDL-PDT, with 18.2 J/cm2 (7 J/cm2 × 2 × 1.3) compared with 37 J/cm2 in cPDT (15), which suggests that additionally doubling the PDL-PDT dose could improve the treatment outcome. In addition, PpIX adsorption is higher at the 630 nm wavelength in cPDT compared with the 595 nm in PDL-PDT (15). Thus, PDL-PDT at 585 nm could be more effective, as was also concluded by Karrer et al. (8). Some studies (11, 14) used multiple treatments 1–2 weeks apart, achieving higher clearance rates. However, a need for multiple treatments would give PDL-PDT a major disadvantage compared with cPDT; based on previous studies cPDT needs one treatment only for AKs (7). Other downsides to PDL-PDT treatment include relatively high costs if the clinic does not currently have a PDL laser device, and operating the device requires expertise.
The current study also shows low clearance rates for the cPDT-treated lesions, with a lesion clearance rate of 73% vs 56–90% in previous studies. The clearance rates were low, even though we differentiated new lesions from persistent ones at follow-up. The study population was mostly severely sun-damaged, which could considerably impact the treatment efficacy. Most of the study patients were attending regular follow-ups at our clinic because of recurrent skin cancers and their precursors. Of the study patients, 78% already had previous treatment for AKs on the treatment area. The mean lesion count in patients was high, at 7.9, and 17% of the patients received treatment for one large field cancerization area. The mean age of the patients, 77.0 years, was higher than in all previous studies (70–73.7). These severely sun-damaged patients are most probably more difficult to treat successfully.
No statistically significant difference was observed in the treatment response for PDL-PDT and cPDT regarding the thicker lesions in grades II–III. However, a lower proportion of only 50% of lesions healed in PDL-PDT vs 61% in cPDT. Not achieving statistical significance could be due to a lower number of lesions in grades II–III (n = 93) than grade I (n = 304). In addition, treatment efficacy is lower overall for thicker lesions, decreasing the possibility of achieving statistical significance.
A limitation of this study is that patients were not blinded to the treatment they received. However, this would be difficult to overcome due to the obvious differences between the 2 illumination methods. The follow-up is rather short, but it is planned to extend the follow-up to 2 years. A further limitation was not to document the mean illumination lengths of the 2 treatment methods or the post-treatment skin reactions. However, the advantages of PDL-PDT treatment regarding these factors have clearly been shown in previous research, where PDL-PDT has been found to be faster and less laborious, and the skin reactions less extensive (9, 10).
This study has a number of major strengths; it has a half-side comparative design, which limits biases, as the patients serve as their own controls. In addition, a blinded investigation is a major strength, as well as the adequate number of study patients and treated lesions. A further strength is that the treated lesions are strictly defined by location, so that new lesions are easily differentiated from persistent ones at the follow-up appointment. In clinical work, as advised by current guidelines (16), we recommend treating the whole photodamaged area at once, although most patients in this study have been treated for distinct lesions. This treatment regimen was chosen to increase the reliability of the study.
This half-side comparative study shows significantly inferior treatment results for PDL-PDT compared with cPDT in a severely sun-damaged population. However, PDL-PDT could serve as a treatment option for patients who are not compliant with cPDT due to its tolerability issues. There is a need for further randomized, comparative and blinded studies on PDL-PDT in the treatment of AKs, preferably on a less sun-damaged population, to ascertain the usability of PDL-PDT. In addition, the most efficient laser parameters and treatment parameters should be determined in further research.
This study was funded entirely by the Clinical Research Institute HUCH Ltd, Helsinki University Hospital’s Inflammation Centre and the Finnish Dermatological Society. None of the grant agencies has influenced the outcome of this paper, and the authors declare no conflicts of interest. The authors warmly thank Timo Pessi, MSc, for performing the statistical analyses and Lasse Ylianttila, MSc, for the light dose calculations.


 Click to show fullsize
Click to show fullsize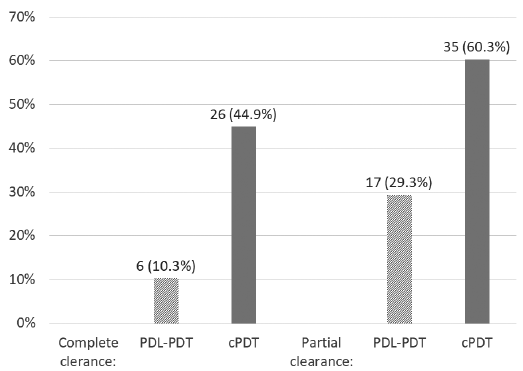 Click to show fullsize
Click to show fullsize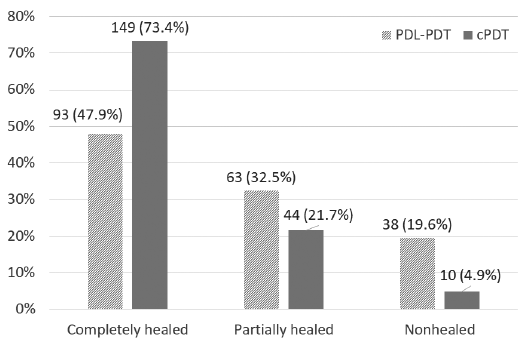 Click to show fullsize
Click to show fullsize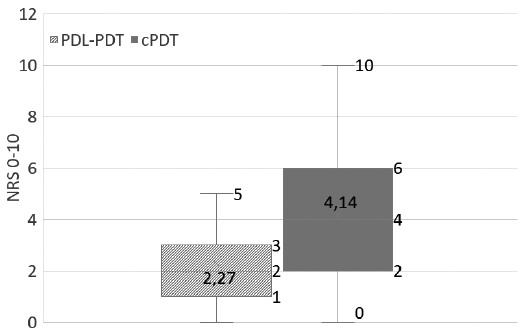 Click to show fullsize
Click to show fullsize