


1Department of Microbiology, Landspítali – The University Hospital of Iceland, 2Faculty of Medicine, University of Iceland, 3Department of Sexually Transmitted Diseases, Landspítali – The University Hospital of Iceland, Reykjavík, Iceland, and 4World Health Organization Collaborating Centre for Gonorrhoea and other Sexually Transmitted Infections, Department of Laboratory Medicine, Faculty of Medicine and Health, Örebro University, Örebro, Sweden
The aims of this study were to assess the prevalence of, and risk factors for, Chlamydia trachomatis in attendees recruited prospectively from October 2018 to January 2019 at the only sexually transmitted infections clinic in Iceland (in Reykjavík), and to evaluate the cobas 4800 CT/NG Test and Aptima Combo 2 Assay for C. trachomatis detection in male urine and female vaginal swabs. Prevalence of C. trachomatis was 15.8% among 487 women and 13.6% among 491 men (no Neisseria gonorrhoeae positive patients were found). C. trachomatis detection was independently and positively associated with being tested for contact tracing, 18–24 years of age, and reporting ≥ 6 sexual partners within 12 months. Reporting sex with non- residents of Iceland was associated with a lower risk of C. trachomatis infection. Both assays had a high sensitivity in detection of C. trachomatis (Aptima Combo 2: 100%; cobas 4800 CT/NG: 95.1%) and high specificity (100% and 99.6%, respectively). The high local prevalence of C. trachomatis and increased acquisition risk following sex with residents are of public health concern.
Key words: Chlamydia trachomatis; Neisseria gonorrhoeae; prevalence; risk factor; nucleic acid amplification; Iceland; sexually transmitted disease.
Accepted Feb 2, 2021; Epub ahead of print Feb 8, 2021
Acta Derm Venereol 2021; 101: adv00393.
doi: 10.2340/00015555-3762
Corr: Ingibjörg Hilmarsdottir, Department of Microbiology, Landspítali – The University Hospital of Iceland, Baronsstigur, 101 Reykjavík, Iceland. E-mail: ingibjh@landspitali.is
The prevalence of, and risk factors for, Chlamydia trachomatis in men and women attending the sexually transmitted infections clinic in Iceland were assessed and diagnostic methods evaluated. Prevalence of Chlamydia trachomatis was 14.7% among 978 participants. Being tested for contact tracing, age range 18–24 years, and reporting ≥ 6 sexual partners within 12 months were associated with higher risk, whereas reporting sex with non-residents of Iceland was associated with a lower risk of Chlamydia trachomatis infection. The cobas 4800 CT/NG Test and Aptima Combo 2 Assay demonstrated high sensitivity and specificity for detection of Chlamydia trachomatis.
Chlamydia trachomatis (CT) and Neisseria gonorrhoeae (NG) cause the 2 most frequently reported bacterial sexually transmitted infections worldwide, which, if not detected and appropriately treated, can result in serious complications and sequelae, such as infertility, ectopic pregnancy and increased HIV transmission (1–3). Programmes for widespread screening or opportunistic testing have offered important insights into the prevalence of, and risk factors for, CT. Prevalence rates of CT in high-income countries are generally below 5% in population-based studies (4), but may exceed 10% in high-risk populations, such as attendees of sexually transmitted infections (STI) clinics (5, 6). Factors that appear to be positively associated with acquisition of CT include young age, high number of sexual partners, inconsistent use of condoms, having a CT-positive sexual partner, previous history of CT infection, being a traveller, and having genital symptoms (1, 6, 7).
Despite an almost 40-year history of CT testing in Iceland (8), a high prevalence among STI clinic attendees (9) and the highest incidence of diagnosed CT in Europe (650 cases per 100,000 population in 2017) (3), no studies have been carried out to understand the sexual behaviour and risk factors for CT acquisition among the local population. In late 2017 the country’s sole STI clinic, at Landspítali (University Hospital of Iceland, Reykjavík), adopted a questionnaire regarding symptoms and sexual behaviour, which is completed by all attendees, thus providing an opportunity for insight into risk factors in our STI clinic population.
Specimens collected for CT/NG screening at Landspítali’s STI clinic have been analysed by the cobas 4800 CT/NG Test (Roche, Basel, Switzerland) since 2017, when the test replaced the Aptima Combo 2 Assay (Hologic Inc., San Diego, CA, USA) at the institution’s Department of Microbiology. Cobas 4800 CT/NG and Aptima Combo 2 are among a handful of nucleic acid amplification tests (NAAT) options adapted to mid or high throughput screening for CT and NG on automated instruments (10). Aptima Combo 2 differs from other assays in that it targets rRNA, which is present in higher numbers in bacterial cells than plasmid or genomic DNA (10). Few studies have compared cobas 4800 CT/NG and Aptima Combo 2 on clinical specimens, and while the latter demonstrated superior sensitivity for CT/NG detection in vaginal and endocervical swabs in one study (10), other reports have found similar sensitivity and specificity of the assays for CT detection in various female and male specimens (2, 11, 12).
The aims of this prospective study were to estimate the prevalence of CT and to identify risk factors for CT in our Icelandic STI clinic population, and compare the diagnostic performance of cobas 4800 CT/NG and Aptima Combo 2.
Patients and biological specimens
Landspítali operates the only STI clinic in Iceland, which has a population of approximately 365,000. The yearly number of CT/NG tested specimens from STI clinic attendees is approximately 6,700, representing approximately a third of all CT and NG tests performed in Landspítali’s Department of Microbiology. From 12 October 2018 to 24 January 2019, all male and female STI attendees who were 18 years of age or older and could complete a standardized questionnaire in Icelandic were invited to enrol in the study. Those who accepted provided informed consent. Medical records were examined for sex and age, and information about symptoms, sexual partners and sexual behaviour was obtained from the standardized questionnaire that is completed by all STI clinic attendees. Men collected first void urine in cobas PCR Urine Sample (Roche) and Aptima Urine Collection tubes (Hologic), and women provided self-collected high vaginal swabs in cobas PCR Media Uniswab Sample (Roche) and Aptima Vaginal Swab Specimen Collection tubes (Hologic). All specimens were tested for CT and NG with the cobas 4800 CT/NG and Aptima Combo 2 assays. Men who had sex with men (MSM), according to patient report, were additionally tested for pharyngeal and anorectal CT and NG infections by the use of cobas 4800 CT/NG, as a part of the routine STI workup. Symptoms compatible with CT infection were defined as dysuria and dyspareunia for both sexes, urethral discharge and symptoms of epididymitis and orchitis in men, and abnormal bleeding and abdominal pain in women (1). The questionnaire item concerning sex with non-residents of Iceland did not distinguish between sex with travellers in Iceland vs sex overseas. Geographical regions were defined according to the United Nations (UN) list (https://unstats.un.org/unsd/methodology/m49/). Assessment of potential risk factors for acquisition of CT was made for men who reported having sex solely with women (MSW) in the 12 months prior to enrolment and women. MSM, defined as men reporting having had sex with men in the 12 months prior to enrolment (irrespective of reported sex with women), differed substantially from MSW and women with regard to condom use and the number of reported sexual partners and non-resident, sexual partners and were therefore not included in the risk factor assessment.
Chlamydia trachomatis/Neisseria gonorrhoeae testing and definition of true-positive results
Specimens collected for the cobas 4800 CT/NG Test, which targets chromosomal DNA in CT (ompA) and NG (2 DR-9 region targets) in addition to cryptic plasmid DNA in CT (12), were stored at room temperature and tested the next workday after specimen collection. Specimen preparation was performed on the cobas x 480 instrument (Roche) and amplification/detection on the cobas z 480 analyser (Roche), according to the manufacturer’s instructions. Specimens collected for the Aptima Combo 2 Assay, which targets 23S rRNA in CT and 16S rRNA in NG (13), were stored at –80°C for a maximum of 3 months until testing at the WHO Collaborating Centre for Gonorrhoea and other Sexually Transmitted Infections at the Örebro University Hospital in Sweden.
Discrepant results between the cobas 4800 CT/NG and Aptima Combo 2 assays were resolved with the singleplex Aptima Chlamydia trachomatis and Aptima Neisseria gonorrhoeae assays (Hologic). In both CT and NG, these assays target species-specific regions in 16S rRNA; for NG the target region differs from the one used in the Aptima Combo 2 assay. All Aptima assays were performed by using the Aptima collection tubes on the Panther instrument (Hologic), according to the manufacturer’s instructions. Results were considered true positive for CT or NG if at least 2 of the 3 assays yielded positive results.
Statistical analysis
Association of CT infection status (positive, negative) with demographic and behavioural characteristics (present, absent) was explored by the use of Fischer’s exact test. Variables that were significantly (p < 0.05) associated with CT and considered clinically relevant risk factors were entered in a multivariable logistic regression model to give an estimate of the effect of each variable, as an adjusted odds ratio (OR) with its 95% confidence interval (95% CI). The fit of the model was assessed with the Hosmer–Lemeshow goodness of fit test. The significance level was set at 0.05. Kappa statistics with values between +1 (perfect agreement) and −1 (complete disagreement) were generated for measure of agreement between the cobas 4800 CT/NG and Aptima Combo 2 assays. Kappa values above 0.8 were considered to indicate very good strength of agreement (14). Stata 13.1 was used for computation.
Ethics
The study was approved by the National Bioethics Committee of Iceland (permission number 18-066).
Demographics and behavioural characteristics.
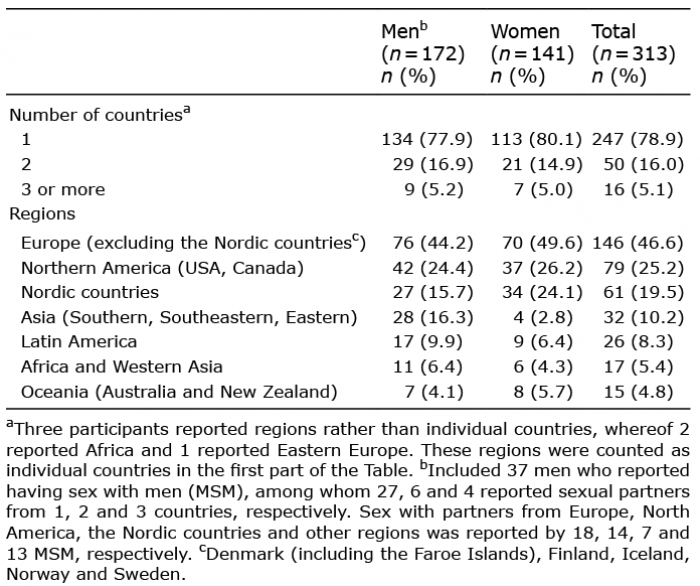
A total of 978 specimens (491 urine and 487 vaginal specimens) from 978 non-duplicate attendees were evaluable and retained for the study. Median age (interquartile range; range) was 25.5 years (22–33; 18–72) for men, 23 years (20–27; 18–70) for women, and 24 years (21–30; 18–72) for all attendees. Among men, 427 were MSW, 57 were MSM, and 7 did not provide information. Reasons for attendance among men and women were STI checkup (participants asymptomatic) for 17.9% and 21.1%, genitourinary or abdominal symptoms for 18.6% and 16.8%, contact tracing (participants with or without symptoms) for 13.3% and 11.5%, and unknown for 0.4% and 0.5%, respectively. The median number of sexual partners during the prior 12 months was 3 for both MSW and women (IQR 2–5; range 1–28 for MSW and 1–30 for women), and 5 for MSM (IQR 3–10; range 1–21). Sex with 6 or more partners during the prior 12 months was reported by 21.7%, 23.1% and 41.5% (22/53), and sex with non-residents during the same period by 30.1%, 33.6% and 73.2% (41/56), of women, MSW and MSM, respectively. Information about the country of origin of non-resident partners was provided by 95.1% of responders (313/329) (Table I). The use of condoms was reported as “always” by 6.7%, 8.2% and 17.9% (10/56) of women, MSW and MSM, respectively. Among MSM this characteristic was seen only in those who reported sex with foreigners; 22.0% of these vs. none of those who reported sex with local residents only used condoms “always”. Past history of STI testing was reported by 77.8% of participants and by 71.8% of those younger than 25 years of age. Past history of STI testing and of CT diagnosis was reported by 80.9% and 42.3% of women, 76.5% and 37.0% of MSW, and 80.4% (45/56) and 27.3% (15/55) of MSM, respectively.
Table I. Number and geographical distribution of countries of non-resident sexual partners as reported by participants for the 12 months prior to enrolment
Chlamydia trachomatis positivity and risk analysis
CT was found in vaginal swabs from 77 women (15.8%) and in urine specimens from 65 MSW and 2 MSM (13.6% for all men); the overall prevalence was 14.7%. In addition, 4 out of 52 MSM who had extragenital specimens taken were CT-positive in 4 anorectal and one pharyngeal specimens (all 4 had CT-negative urine specimens), thus bringing the CT prevalence to 11.5% (6/52) among the participating MSM. No true NG-positive patient was found.
Univariate analysis of 914 women and MSW (Table SI) found significantly higher CT prevalence among participants reporting symptoms compatible with CT infection compared with those with no or other symptoms (21.1% vs 13.4%; p = 0.02) (Table SI); however, this was explained by a strong association with symptoms in MSW (no association in women). Significant, positive association with CT infection was also found for the following variables, and for both sexes, unless otherwise specified: (i) contact tracing as a reason for attending compared with other reasons (28.3% vs 11.1%; p < 0.001); (ii) the age group 18–24 years compared with 35–72 years (20.0% vs 5.8%; p < 0.001) and the age group 25–34 years compared with 35–72 years for MSW but not for women; and (iii) reporting sex with 6 or more partners in the previous 12 months compared with sex with fewer partners (25.1% vs 12.7%; p < 0.001), although this variable was positively associated with CT for women only. A lower risk for CT positivity was found for attendees reporting sex with non-residents in the previous 12 months compared with those reporting sex solely with residents of Iceland (9.8% vs 18.3%; p < 0.001) and this was seen for both women and MSW. Previous history of STI testing, or of having tested positive for any STI or for CT, were not significantly associated with CT infection in our population (Table II and Table SI).
Table II. Demographic and behavioural characteristics associated with Chlamydia trachomatis positivity in univariable and multivariable model analyses of women and men who have sex with women
The abovementioned variables, except for symptoms, were entered into the multivariable model; symptoms were not used because they are expected to result from CT infection rather than affect risk of acquisition. Data for a total of 884 women and MSW were used in the model, which showed the 4 variables to be independently associated with increased or decreased risk of CT positivity (Table II); interaction between variables was non-significant (in accordance with the linktest in Stata).
Comparison of cobas 4800 CT/NG and Aptima Combo 2
True-positive CT results were obtained by cobas 4800 CT/NG and Aptima Combo 2 for 137 and 144 specimens, respectively (Table III). The singleplex Aptima Chlamydia trachomatis was used to resolve discrepancy for 10 specimens, and results were identical to the Aptima Combo 2 results. The sensitivity of Aptima Combo 2 and cobas 4800 CT/NG for the detection of CT was 100.0% and 95.1%, respectively; a kappa value of 0.959 indicated very good agreement between the methods for the 978 specimens. Overall specificity was comparable, i.e. 100% and 99.6%, respectively.
Table III. Diagnostic performance of cobas 4800 CT/NG (Roche) and Aptima Combo 2 (Hologic) in the detection of Chlamydia trachomatis
The nationwide incidence of CT and the prevalence among STI attendees have remained stably high in Iceland since 1996 (when detection by PCR was introduced at Landspítali) despite universal access to healthcare and free STI testing. From 1997 through 2018, the annual incidence ranged from 524 to 736 per 100,000 population (15), and Iceland had the highest incidence of diagnosed CT in Europe during the period of 2010 to 2017, with 529–692 cases per 100,000 population reported annually (3). The prevalence of CT was 13.9% among men and women attending Landspítali’s STI clinic in 1996 (9), and thus comparable to the 14.7% found in the present study (based on urine and vaginal swab testing). Recent and similarly designed studies from STI clinics or comparable providers in the Nordic countries, Germany, the Netherlands, Canada, USA and Australia, have shown prevalence rates ranging from 4.1% to 10.8% (5–7, 10, 12, 16–18). The high rate of previous STI testing reported by the study population (77.8%) suggests reliance on easy access to healthcare and testing availability for control of CT infection, rather than preventive sexual behaviour, such as condom use and limiting the number of partners. In a recent Swedish study, previous CT testing appeared to have a significant and strong “protective effect” against CT infection (6); however, no such association was found in our population for previous STI testing.
The absence of diagnosed NG infections among our participants is probably explained by the low overall prevalence in the country, i.e. 29.8 cases per 100,000 population in 2018 (19). In addition, the majority of cases during the past decade have corresponded to male patients (83% were males in 2018) (19), many of whom are expected to be MSM (20).
CT prevalence was independently associated with young age (18–24 years) and with a high number of sexual partners, both of which have previously shown an association with CT infection (6, 7). The role of age, however, was challenged in a recent cohort study in which age, up to 32 years, was not an independent factor for CT infection after accounting for partner numbers, and in older individuals the risk declined only for women (21).
An unexpected finding of the current study was that engaging in sex with non-residents of Iceland was associated with a lower risk for CT infection compared with having sex with the local population only (9.8% vs 18.3%). Travel is a recognized risk factor for STI acquisition, which could be related to higher STI prevalence rates in some countries and increased risk-taking behaviour, such as casual sex (22). Thus, a large Australian study found prevalence of CT to be significantly higher in travellers to Australia (11.2%) than in residents (8.5%) (7). One might therefore have expected a higher CT prevalence among participants who engaged in sex with non-residents of Iceland. The current study did not collect information about whether sexual encounters took place locally or abroad, but, given the large number of foreign visitors in Iceland (more than 2 million in 2018) (23) and high outbound travel propensity among local residents (almost 80% travelling abroad in 2017 according to a recent a survey (24)) we assume that both scenarios were common among our participants. We speculate that frequent change of partners, combined with unprotected sex among members of the small Icelandic community, where the incidence of CT is elevated, probably explains the high prevalence of CT for the group reporting sex with local residents only.
A high overall agreement for true-positive and true-negative CT results (99.0%, 973/983) was found between cobas 4800 CT/NG and Aptima Combo 2, and the negative predictive value of cobas 4800 exceeded 99% overall despite a high prevalence of CT. We are aware of only 5 studies that have compared the performance of cobas 4800 CT/NG and Aptima Combo 2 by using the same set of specimens in the investigator and comparator assays (2, 10–12, 25). Their design differed from that used in the current study, in that all specimens were tested with 3 different NAAT assays (compared with 2 in ours), and in all but one of the studies (25) the definition of true-positive and true-negative results was based on the patient infected status (PIS), which required concordant results from at least 2 out of 3 assays for any specimen type from the same patient. Four of these studies found sensitivity values for CT detection on cobas 4800 CT/NG to be 84.6–97.6% for vaginal swabs, 91.6–93.6% for endocervical swabs, 92.3–93.8% for female urine, and 97.6–98.4% for male urine (2, 10–12). Specificity values for the different specimen types on cobas 4800 were consistently high, i.e. 99.2–100% (2, 10–12). Although the rRNA-based Aptima assay could be expected to demonstrate enhanced sensitivity over DNA-based comparator assays the performance of cobas 4800 CT/NG was largely comparable to Aptima Combo 2 in the 4 studies, with the exception of one (10) in which a significantly lower sensitivity was observed for vaginal swabs on cobas 4800. The fifth study (25) found 99.4–100% overall agreement between cobas 4800 CT/NG and Aptima Combo 2 for CT detection in male and female urine and 96.8% agreement for endocervical swabs; cobas 4800 detected CT in 98.3–100% of urine and 83.5% of endocervical swabs that were Aptima positive. In addition to the 5 studies discussed above, van der Pol et al. (26) found 92.9% sensitivity and 99.7–99.8% specificity for CT detection in vaginal swabs on cobas 4800 CT/NG when results were compared with a PIS based on urine and endocervical swabs tested with Aptima Combo 2 and the BD ProbeTec CT/GC QxAmplified DNA Assay (BD).
Study limitations
The study included some limitations. First, because women were not systematically tested for vaginal infections, which may cause dysuria and dyspareunia, the evaluation of CT infection as a potential cause of symptoms in women was not possible. Secondly, as participation was voluntary it is possible that attendees with symptoms or high-risk behaviour were more likely to participate, which might have increased the prevalence of CT. However, since all attendees of the STI clinic are tested for CT/NG, irrespective of an ongoing research study, it is unlikely that participation significantly biased the CT prevalence observed. Furthermore, since participation was voluntary in most of the studies referred to regarding CT prevalence, we believe that the difference in prevalence observed between Iceland and other countries is real (6, 7, 10, 12, 16, 18).
Conclusion
The consistently high prevalence of CT infection in the Icelandic STI clinic population, despite easy access to healthcare and testing, is probably a result of liberal sexual morals, low rate of condom use and a high incidence of CT in the community. An unexpected finding was the significantly lower risk for CT infection when engaging in sex with non-residents compared with having sex solely with the local population, and this merits further investigation with potential implications for public health approaches. The cobas 4800 CT/NG Test was highly sensitive for detection of CT, compared with the Aptima Combo 2 Assay, and retained an excellent negative predictive value in the high-prevalence population in this study.
This work was supported by grants from Landspítali University Hospital, the Örebro County Council Research Committee, and the Foundation for Medical Research at Örebro University Hospital.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize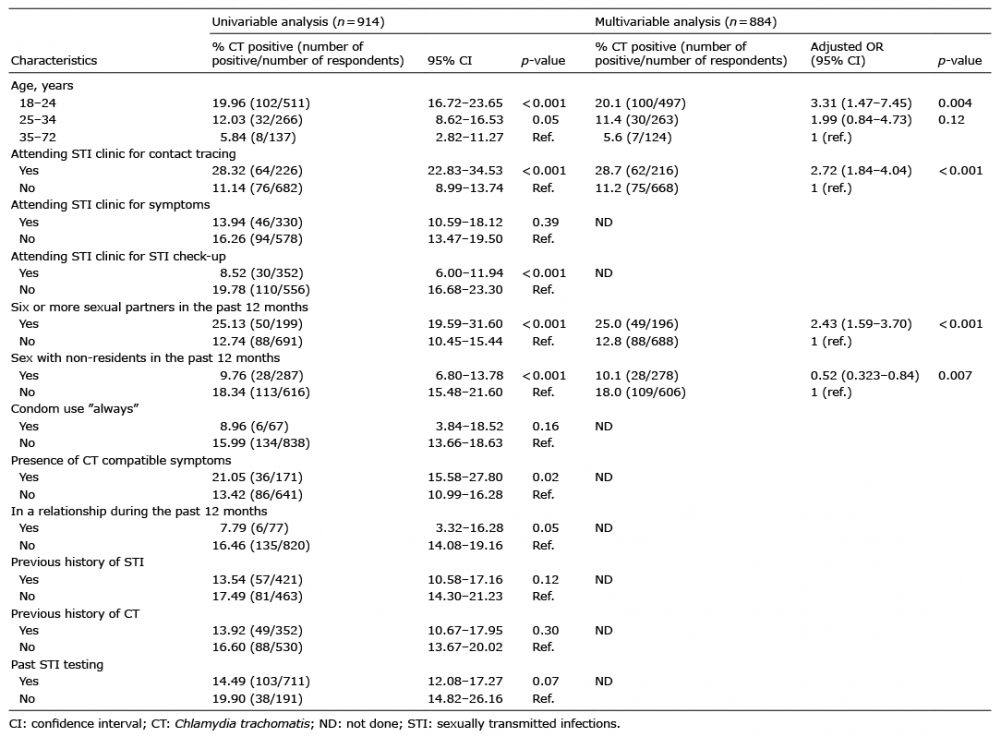 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize