


1Section of Dermatology, Department of Medicine, 2Section of Pathology, Department of Diagnostics and Public Health, University of Verona, IT-37126 Verona, Italy. E-mail: giacomo.dalbello@studenti.univr.it
A 42-year-old woman presented with a brown recluse spider (Loxosceles reclusa) venom bite on her left thigh. At first, she presented erythema with pain at the site of spider bite, subsequently a vesicular-bullous lesion appeared evolving into a ulcero-necrotic area associated with lymphangitis. She was treated with topical and systemic antibiotics, which resulted in improvement in her condition. Subsequently, she presented 5 recurrent non-movable, firm, deep-seated nodules on her left thigh for approximately one year (Fig. 1). She was apparently healthy, and her past medical and family histories were not contributory. One lesion with a diameter of approximately 10 mm was surgically removed by excisional biopsy.
What is your diagnosis? See next page for answer.
Fig. 1. Five mobile deep-seated nodules on the left thigh.
Acta Derm Venereol 2021; 101: adv00400.
Diagnosis: Nodular cystic fat necrosis due to brown recluse spider venom bite
Histopathological examination revealed extensive fat necrosis composed of numerous unilocular cystic spaces of various sizes rimmed by histiocytes; the cystic spaces were sometimes surrounded by condensed fibrous tissue with lipomembranous change and dystrophic calcification. Pearls negative brownish pigment, thought to be foreign materials were seen around the fully developed stage of fat necrosis (Fig. 2). Based on the above clinical and histopathological findings, a diagnosis of nodular cystic fat necrosis due to brown recluse spider venom acupuncture was made.
Nodular cystic fat necrosis, first described by Pryjemski & Schuster (1) in 1978, is a benign condition characterized by encapsulated fat necrosis. This condition is not uncommon, but is probably not commonly recognized and a histological examination is seldom performed. Nodular cystic fat necrosis has been reported to be associated with erythema nodosum, Heerfordt’s syndrome, systemic sclerosis, lupus erythematosus and IgA nephropathy (2). The lesion may be solitary or multiple and is usually located on sites vulnerable to trauma, especially in the lower extremities (3). Histologically, it is characterized by localized encapsulated fat necrosis with a pseudo-cystic cavity. Some authors have suggested that these lesions are related to vascular insufficiency and trauma, but cases without any trauma history, with subsequent fat necrosis and fibrous encapsulation, have been described (4). Some authors have hypothesized that calcification of fat tissue is related to altered blood supply due to mechanical interference by fibrosis or torsion, and nodules may undergo coagulative necrosis. Once the fat cell is damaged, triglycerides undergo hydrolysis into glycerol and fatty acid; fatty acids combine with calcium, resulting in calcification of the fat. The relatively avascular structure of the cyst wall precludes complete resorption of cyst fluid and organization of loose bodies (1). Lipomembranous changes are uncommon patterns of fat necrosis caused by a wide variety of local or systemic events that may compromise blood supply of the subcutaneous tissue (3). In end-stage lesions, fibrosis and dystrophic calcification are seen within the encapsulated nodules (5). Another similar case of nodular cystic fat necrosis due to insect venom acupuncture, via bee acupuncture, has been described by Yoonseok et al. (6).
In conclusion, we report here a case of nodular cystic fat necrosis showing calcification and lipomembranous changes due to brown recluse spider venom acupuncture. Nodular cystic fat necrosis is not an uncommon condition, but it is often either diagnosed only descriptively or confused with other lesions, such as lipomas, phleboliths, lipodermatosclerosis, and calcinosis cutis.
Fig. 2. (a) Fat necrosis with unilocular cystic spaces of various sizes (haematoxylin and eosin staining ×100 magnification). (b) Some cystic spaces surrounded by condensed fibrous tissue with lipomembranous change (Alcian blue and periodic-acid Schiff (PAS) staining ×500 magnification).


 Click to show fullsize
Click to show fullsize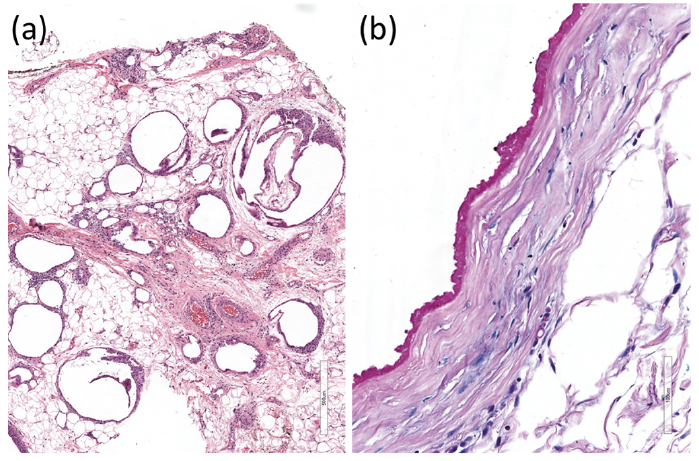 Click to show fullsize
Click to show fullsize