


Adam Reich1, Monika Kobierzycka1, Zdzisław Woźniak2, Maria Cisło1 and Jacek C Szepietowski1
Departments of 1Dermatology, Venereology and Allergology and 2Pathology, University of Medicine, Ul. Chalubinskiego 1, PL-50-368 Wroclaw, Poland. E-mail: adi_medicalis@go2.pl
Accepted April 20, 2006.
Sir,
We present a patient with a keratoacanthoma-like manifestation of cutaneous metastasis, which lead to detection of lung cancer. To the best of our knowledge this is the first such description regarding lung carcinoma.
CASE REPORT
A 58-year-old woman was admitted to our department with a tumour of the scalp. On admission, a 4 cm diameter, round, hard, red tumour with a central keratin plug was observed. During the 10-month period of development of the lesion no ulceration was seen within the tumour. The lesion clinically resembled keratoacanthoma (Fig. 1). Moreover, enlargement of the right supraclavicular lymph node was diagnosed.

Fig. 1. A round, 4 cm diameter tumour with central keratin plug located on the scalp, which clinically resembled keratoacanthoma.
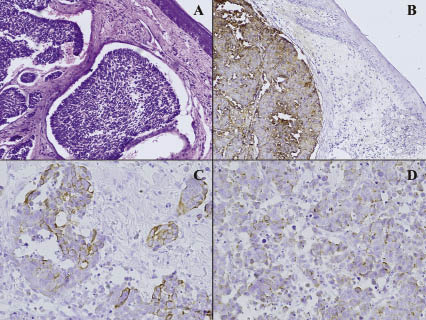
The patient has also suffered from psoriasis vulgaris, which had been treated in the past with topical agents, including tar preparations and phototherapy (narrowband UVB 311 nm). Moreover, she smoked more than 40 cigarettes per day for over 20 years. Biopsy of the skin lesion surprisingly revealed a metastatic carcinoma consisting of intermediate cells (Fig. 2A). The tumour cells were positive for epithelial membrane antigen (Fig. 2B), CAM 5.2 pancytokeratin marker (Fig. 2C) and chromogranin A (Fig. 2D). Moreover, metastases were also detected in the excised lymph node. Additionally, histological examination confirmed that the central plug consisted mainly of keratin and epithelial cells.
On admission, routine laboratory examination revealed slight leukocytosis (10500/mm3), hyperglycaemia
(125 mg%), hypertriglyceridaemia (243 mg%) and hypomagnesaemia (0.6 mmol/l). The serum level of carcinoembryonic antigen was very high (164.6 ng/ml, normal value <2.5 ng/ml). Sonography of the abdomen revealed hepatomegaly and splenomegaly. Computed tomography scan of the thorax revealed a small tumour (2.5×1.8 cm) in the apex of the right lung and enlargement of the paratracheal lymph nodes. Biopsy of the lung during bronchoscopy confirmed the diagnosis of lung cancer with metastases to the skin and lymph nodes.
Fig. 2. (A) Histology: metastatic carcinoma consisting of intermediate cells (haematoxylin and eosin (H&E), original magnification ×100); (B) Positive reaction for EMA (epithelial membrane antigen); (C) Positive reaction of tumour cells for pancytokeratin marker; (D) Positive reaction of tumour cells for chromogranin A. (Immunochemistry, B: ×100, C: ×200, D: ×200).
DISCUSSION
Clinical manifestation of cutaneous metastases
mimicking keratoacanthoma are very unusual and seldom reported. Until now there have been only two such descriptions in the literature: one in mesothelioma (1) and one in soft tissue mesenchymal chondrosarcoma (2). Moreover, keratoacanthoma-like lesions were also found to be squamous cell carcinoma (3). Additionally, there is one report of primary cutaneous CD30+ anaplastic large cell lymphoma of keratoacanthoma-like presentation (4). In the patient presented here, the diagnosis of keratoacanthoma was very probable. The lesion was found on the scalp, the area with many hair follicles, from which keratoacanthoma is suggested to arise. Moreover, the
patient had a long history of smoking as well as of treatment with tar and phototherapy – factors which are known to induce the development of keratoacanthoma. However, because of the size of the lesion (4 cm diameter) a skin biopsy was performed, which revealed the metastatic character of the skin lesion. It is worth emphasizing that the patient had not previously been diagnosed as having carcinoma and the presence of the skin lesion lead to detection of malignancy.
REFERENCES
1. Cassarino DS, Xu W, Shannon KJ. Widespread cutaneous and perioral metastases of mesothelioma. J Cutan Pathol 2003; 30: 582–585.
2. Aramburu-Gonzalez JA, Rodriguez-Justo M, Jimenez-Reyes J, Santonja C. A case of soft tissue mesenchymal chondrosarcoma metastatic to skin, clinically mimicking
keratoacanthoma. Am J Dermatopathol 1999; 21: 392–394.
3. Schwartz RA, Tarlow MM, Lambert WC. Keratoacanthoma-like squamous cell carcinoma within the fibroepithelial polyp. Dermatol Surg 2004; 30: 349–350.
4. Lin JH, Lee JY. Primary cutaneous CD30 anaplastic large cell lymphoma with keratoacanthoma-like pseudocarcinomatous hyperplasia and marked eosinophilia and neutrophilia. J Cutan Pathol 2004; 31: 458–461.

