


Sir,
Chronic graft-versus-host disease (GVHD) involving the vulva or vagina has been reported in 15% of females receiving allogeneic peripheral stem cells (1–3). We have, however, been unable to find any reports of genital GVHD in men. Here we describe the case of a man who developed chronic GVHD with severe genital involvement.
CASE REPORT
A 61-year-old man was diagnosed with refractory anaemia with an excess of blasts. Allogeneic peripheral blood stem cell transplantation with an unrelated donor was performed 2 years later after reduced intensity conditioning with busulphan, fludarabine and anti-thymocyte globulin. Short-term methotrexate and cyclosporine were given as GVHD prophylaxis. The post-transplant period was uneventful, but mixed chimerism with 12% recipient myeloid cells was noted and immunosuppressive prophylaxis stopped after 3 months. Three weeks later he had developed skin GVHD stage 2 that responded to short-term treatment with oral corticosteroids. One month later he also had hepatic GVHD grade 2, and full donor chimerism was established. After re-institution of cyclosporine and corticosteroids the skin symptoms resolved and bilirubin and aminotransferase levels normalized. Cyclosporine treatment was continued, and at routine check-up 4 months later he was in good health with normal blood counts and hepatic enzymes. There was no cutaneous GVHD, but asymptomatic lichenoid lesions were seen on oral examination. The patient had no complaints and denied genital symptoms, but at physical examination lichenoid genital lesions were seen.
The prepuce was somewhat narrowed and on the distal prepuce and the glans there were glazing erythema and erosions. On the skin surrounding the frenulum and underneath the penis there were changes resembling lichen sclerosus (Fig. 1).
Fig. 1. Genital examination revealed lichenoid genital lesions.

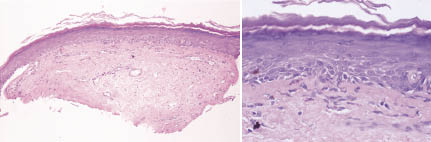
A skin biopsy from the prepuce was obtained and stained with haematoxylin (Fig. 2). The epithelium was seen to be split from the connective tissue, probably due to immune-complex induced damage. The epithelium showed hyperkeratosis and hypergranulosis. The rete pegs were generally flattened, but focally small signs of irregular acanthosis could be seen. A few scattered apoptotic keratinocytes were seen, as well as focal signs of basal cell degeneration. There was no cellular atypia. The connective tissue was slightly fibrotic with a few dilated small vessels, but there was no inflammatory reaction or vasculitis. The histological picture was compatible with chronic GVHD, although morphea and systemic sclerosis are differential diagnoses. However, given the patient’s history and the fact that he also had hepatic and cutaneous GVHD in other areas, as well as oral GVHD, chronic GVHD is the most likely diagnosis.
Fig. 2. Biopsy showed that the epithelium was split from the connective tissue and the rete pegs were generally flattened. A few scattered apoptotic keratinocytes were seen, as well as focal signs of basal cell degeneration. The connective tissue was slightly fibrotic, but there was no inflammatory reaction or vasculitis. The histological picture was compatible with chronic graft-versus-host disease.
The patient was treated with a topical steroid ointment (betametason) combined with neomycin on a regular basis for some weeks. At follow-up 4 months later the inflammation had almost completely disappeared, there was no longer any moisturing and the prepuce had adhered to the glans as seen in erosive lichen planus and plasma cell balanitis (Fig. 3).
Fig. 3. At follow-up the inflammation had disappeared.

DISCUSSION
Genital manifestations of chronic GVHD are common among females, but there are no reports about their frequency among male allogeneic stem cell transplant recipients. We want to stress the similarities between GVHD and erosive lichen planus. Clinically it is often difficult or impossible to differ between lichen planus and GVHD localized to oral and genital mucosa. Histologically they also seem to be almost identical. The immunopathogenesis of lichen planus is not fully understood, but there is evidence for the role of T-lymphocytes, which are also involved in GVHD.
It is also worth noting that genital problems are often concealed or denied by the patient and may be overlooked if the physical examination does not include the genital area. We therefore emphasize the need to examine the whole patient, including the genital area, and that proper treatment of these patients requires team work with a multidisciplinary approach (4).
REFERENCES
1. Spinelli S, Chiodi S, Costantini S, Van Lint MT, Raiola AM, Ravera GB, Bacigalupo A. Female genital tract graft-versus-host disease following allogeneic bone marrow transplantation. Haematologica 2003; 88: 1163–1168.
2. Chiodi S, Spinelli S, Abraham G. Sexual problems after allogenic stem cell transplantation. Rev Med Suisse 2006; 2: 779–780, 782–783.
3. Lee SJ, Vogelsang G, Gilman A, Weisdorf DJ, Pavletic S, Antin JH, et al. A survey of diagnosis, management, and grading of chronic GVHD. Biol Blood Marrow Transplant 2002; 8: 32–39.
4. Couriel D, Carpenter PA, Cutler C, Bolanos-Meade J, Treister NS, Gea-Banacloche J, et al. Ancillary therapy and supportive care of chronic graft-versus-host disease: national institutes of health consensus development project on criteria for clinical trials in chronic Graft-versus-host disease: V. Ancillary Therapy and Supportive Care Working Group Report. Biol Blood Marrow Transplant 2006; 12: 375–396.
Elisabet Nylander1, Ylva Britt Wahlin2, Bertil Lundskog3 and Anders Wahlin4
Departments of 1Clinical Medicine and Public Health/Dermatology and Venereology, 2Odontology, 3Medical Bioscience/Pathology and 4Clinical Medicine and Public Health/Medicine, Umeå University, SE-901 85 Umeå, Sweden. E-mail: Elisabet.Nylander@vll.se
Accepted November 14, 2006.

