Vulvar vestibulitis is a major cause of entry dyspareunia in young women. The aim of this study was to evaluate a self-reported history of bacterial vaginosis, candidiasis, use of oral contraception and nulli-pregnancy as risk factors for vestibulitis. A retrospective examination of medical records was performed for 45 patients with vestibulitis from a vulvar clinic in Oslo, median age 24 years, age range 19–49 years. Four controls per case were selected randomly from the same Oslo source population as the cases. Age-matching was not performed, as matching does not control for confounding in the case-control design. Controls anonymously answered a postal questionnaire, response rate 61%. The crude effect for the major potential predictors for vulvar vestibulitis was estimated, and stratification on age for the major potential predictors. The method of Mantel Haenszel was used to quantify confounders, and control for multi-confounders and the gradient effect of different covariates was performed. The major confounder was age. Independent risk factors for vestibulitis were nulli-pregnancy, odds ratio (OR) 8.4 (95% confidence interval (CI) 2.8–25.2) and bacterial vaginosis, OR 3.37 (95% CI 1.06–10.6). Adjusting for age diluted the effect of oral contraception and frequent treatment for candidiasis. This study is the third case-control study identifying bacterial vaginosis as a risk factor for vestibulitis. Thus, it remains to be investigated whether abnormal vulvo-vaginal microbiota belongs to the aetiology of vulvar vestibulitis. Key words: vulvar vestibulitis; case-control study; oral contraception; genital infections; bacterial vaginosis.
(Accepted December 21, 2006.)
Acta Derm Venereol 2007; 87: 350–354.
Karin Edgardh, Sesam City, Department of Obstetrics and Gynecology, Karolinska University Hospital, Stockholm, Sweden. E-mail:karinedgardh@yahoo.se
Vulvar vestibulitis is a major cause of vulvodynia in young women. The condition is diagnosed by use of Friedrich’s criteria from 1987 (1): longstanding and severe pain on vestibular touch or attempted vaginal entry, tenderness in response to pressure localized within the vulvar vestibule (the cotton swab test) and physical findings confined to vestibular erythema of various degrees. The major symptom, entry dyspareunia, is reported to be increasing, especially among young women. In a Swedish population-based study by Danielsson et al. (2), 13% of 20–29-year-olds reported a history of longstanding superficial dyspareunia, compared with 6.5% of 50–60-year-olds.
Vestibulitis is not an inflammation in its classical sense, as found by Lundqvist et al. (3) and Bohm-Starke et al. (4, 5), but is recognized as a pain syndrome. The pathophysiology is currently understood as vestibular nociceptor sensitization, i.e. activation of C-type fibres and an abnormal firing in neurones in the dorsal root horn. Thus, the terms “vestibulitis” or “vulvar vestibulitis syndrome” are to be replaced by “localized vulvar dysaesthesia” or “localized provoked vulvodynia” (6). However, “vestibulitis”, or “vulvar vestibulitis syndrome” (VVS), are still common terms, and thus are used in this paper. A state-of-the-art consensus on definitions, diagnosis and management was published recently by a group of international experts within the field of vulvodynia (7).
Vestibulitis is considered a multifactorial condition, and a number of case-control studies have been published on possible risk factors. Danielsson et al. (8) have focused on psychosomatic factors, Nylander Lundqvist & Bergdahl (9) on depression. In 1997, Sjöberg et al. (10) and in 2002, Bouchard et al. (11) reported use of oral contraception to have a role in the development of vestibulitis. In 1999, Sarma et al. (12) and in 2002 Smith et al. (13) found bacterial vaginosis and vulvo-vaginal candidiasis to belong to the independent risk factors for VVS. Infection with human papilloma virus (HPV), has been investigated, but has not been found to be a consistent risk factor (12–15).
In 2003, longstanding entry dyspareunia was reported by 6.9% of 502 consecutive drop-in female patients at the Olafia centre for sexually transmitted infections (STI) in Oslo (16). The study was based on patients’ self-reports, and did not include clinical findings and diagnoses. Patients often came to the centre due to their pain problems, in spite of not suspecting a STI. A history of bacterial vaginosis and frequent treatment for vulvo-vaginal candidiasis were independent risk factors for entry dyspareunia, whereas STI and use of oral contraception were not. The aim of the present study was to evaluate whether these factors were also related to vulvar vestibulitis, in a population-based case-control study in the same city.
MATERIALS AND METHODS
Case and control definitions
During the period January 2000 to March 2003, 50 of 217 patients referred to the vulvar clinic at the Olafia centre for STIs in Oslo had a first diagnosis of vestibulitis, according to Friedrich’s criteria (1). The clinic was, at the time, the only one in Oslo dedicated to vulva patients, and was run by the author KE. Of all 50 patients, 45 lived in greater Oslo and were chosen as cases. A retrospective examination of medical records was performed by KE, with regard to sociodemographic data, age at coitarche, use of oral contraception, pregnancy and parity, and history of genital infections. Causes of entry dyspareunia, other than vestibulitis, were excluded. Data were summarized into a case report form (CRF). Thus, all patients were examined by KE, and the medical records were revised by KE. The patients’ median age was 24 years, range 19–49 years.
Four controls per case were selected randomly from the same source population as the cases, i.e. women aged 16–49 years from greater Oslo. Random sampling from the national registration was made by Statistics Norway. A self-administered questionnaire including 25 items on the same topics as in the patients’ CRFs was posted to the controls. Two reminders were issued. All post, i.e. information letters and the questionnaire, was handled by Statistics Norway. Data were collected during the period August 2003 to November 2003. The participants were anonymous to the investigators KE and MA.
The study was approved by the local ethics committee.
Power estimation
The prevalence of bacterial vaginosis (BV) was estimated to be 24% in the control group. The estimate was based on a Norwegian prevalence study (17). We hypothesized a three times higher frequency of a history of BV in patients with vestibulitis than among controls (odds ratio (OR) = 3). With four controls for every case, a type I error of 5% and a power of 80%, 40 cases and 160 controls were required. We included all 45 cases, and thus chose 180 controls.
Statistical analysis
Crude effect for the major potential predictors for VVS was estimated by the OR, and its 95% confidence interval. As age would be a strong confounder, a stratification on age was performed for the major potential predictors for VVS. The method of Mantel Haenszel was used to quantify confounders by comparing the crude ORc with the adjusted Mantel Haenszel odds ratio (ORmh). In order to pinpoint effect modification we compared OR in the different strata. The Breslow and Day test of heterogeneity was used to highlight heterogeneity in the different strata (18, 19). Control for multi-confounders was performed using the logistic multivariate model (18). Age-matching was not performed, as matching does not control for confounding in the case-control design (18–20). The gradient effect of different covariates on the frequency of vestibulitis was estimated by the extended Mantel Haenszel χ2 test for linear trend (20).
RESULTS
Response rate
The planned number of controls was four per case, but only 130 controls participated; a response rate of 61%. The major effect of this low response rate was a power diminution of the study.
Drop-outs did not differ from responding controls with regard to age and place of residence. However, 27 of the 130 controls (20.8%) reported current entry dyspareunia, and were excluded from the analyses.
Table I presents the results in a univariate analysis, with crude effects of investigated risk-factors. Cases were significantly younger than controls, 25 years vs. 35 years. No statistically significant difference was found between age at first intercourse. Current use of oral contraception (OC) carried an excess risk of vestibulitis, compared with non-use of OC, OR=2.9, p=0.004. Never having been pregnant was also related to vestibulitis, OR=16.5, p <0.0001. A history of STI, i.e. genital chlamydia, herpes or condylomas, did not differ between cases and controls, neither did candidiasis and bacterial vaginosis.
Table I. Frequencies of major variables in cases of vulvar vestibulitis and controls
| Variables | Cases n = 45 | Controls n = 103 | p-value | OR | 95% CI |
| Age at onset of the study (years) | 25 SD = 5.5 | 35 SD = 7.14 | 0.001 | | |
| Married/cohabiting | 20 | 48 | 0.29 | 0.9 | 0.4–1.8 |
| Age at first intercourse (years) | 15.8 SD = 6 | 17.2 SD = 4.2 | 0.123 | | |
| Oral contraception (OC) |
| Current use of OC | 20 | 22 | 0.004 | 2.94 | 1.4–6.2 |
| Total time of OC use (years) | 4.4 SD = 6.3 | 5.3 SD = 4.9 | 0.11 | | |
| Pregnancy |
| Never pregnant | 39 | 29 | < 0.0001 | 16.5 | 6.3–43.2 |
| History of genital infections |
| Chlamydia | 6 | 24 | 0.165 | 0.5 | 0.19–1.3 |
| Herpes | 4 | 5 | 0.353 | 1.8 | 0.5–7.4 |
| Condylomas | 4 | 3 | 0.122 | 3.1 | 0.6–14.0 |
| Candidiasis, single episode | 36 | 72 | 0.20 | 1.7 | 0.7–4.0 |
| Candidiasis, treatment > 10 times | 8 | 16 | 0.30 | 1.14 | 0.45–2.8 |
| Bacterial vaginosis | 14 | 23 | 0.30 | 1.57 | 0.71–3.4 |
Mean and SD: standard deviation; OR: odds ratio, and 95% confidence interval (CI); Cases: cases of vestibulitis.
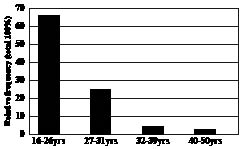
In Fig. 1, we have polythomized the continuous variable age in quartiles. The frequency of VVS was decreasing with age, and the effect of age on vestibulitis also showed a dose response nature, as the extended test of Mantel Haenszel of linear trend was highly significant (p=0.00001). In Table II, the same pattern was shown for number of pregnancies, where a significant gradient effect was found, p ≤00001. The same pattern occurred significantly between the number of births and the frequency of VVS.
Fig. 1. Age and frequency of vulvar vestibulitis syndrome (VVS).
Table II. Gradient effect of the number of pregnancies on the frequency of vulvar vestibulitis syndrome (VVS) using the Mantel-Haenszel test of linear trend
| VVS | No. of pregnancies |
| 0 | 1 | ≥2 | Total |
| Yes | 41 | 2 | 2 | 45 |
| No | 32 | 20 | 51 | 103 |
| Total | 73 | 22 | 53 | 148 |
| Frequency (%) | 56.1 | 9.0 | 3.7 | |
| OR | 32.6 | 2.55 | 1.0 | |
| 95% CI | 6.9–210 | 0.2–2.7 | | |
OR: odds ratio; CI: confidence interval.
Mantel-Haenszel test of linear trend χ2 = 41.2 and p <0.00001.
Thus, age was associated with the occurrence of vestibulitis and highly associated with the use of OC and a history of pregnancies. Consequently, age was the major confounder to be controlled. Table III shows the results of a stratification analysis using the Mantel-Haenszel method to quantify confounding effects and pinpoint effect modification. The confounding effect was estimated by comparing the ORc with the ORmh. Adjusting for age diluted the effect of current use of OC and lowered the effect of nulli-pregnancy on the occurrence of vestibulitis. On the other hand, it increased the effects of a history of frequent treatment of candidiasis and bacterial vaginosis.
Table III. Risk factors for vulvar vestibulitis syndrome (vvs), adjusted on age groups, by stratification and using the Mantel-Haenszel method
| Variable | 16–31 years VVS No | 16–31 years VVS Yes | 32–49 years VVS No | 32–49 years VVS Yes | ORmh | 95% CI | Breslow Day p = value |
| Married/cohabiting No Yes | 24 8 | 25 17 | 31 40 | 0 3 | 2.5 | 0.94–6.5 | 0.299 |
| Current oral contraception No Yes | 17 15 | 23 19 | 64 7 | 2 | 1.07 | 0.4–2.6 | 0.213 |
| Never pregnant No Yes | 12 20 | 5 37 | 62 9 | 1 2 | 5.21 | 1.8–15.1 | 0.407 |
| Genital chlamydial infection No Yes | 25 6 | 36 6 | 53 18 | 3 0 | 0.55 | 0.16–1.8 | 0.350 |
| Genital herpes infection No Yes | 29 2 | 38 4 | 68 3 | 3 0 | 1.36 | 0.2–7.4 | 0.658 |
| Condylomas No Yes | 29 1 | 38 4 | 69 2 | 3 0 | 0.62 | 0.3–21.4 | 0.62 |
| Treatment for candidiasis > 10 times No Yes | 12 20 | 9 33 | 19 52 | 0 3 | 2.51 | 0.9–6.9 | 0.480 |
| Bacterial vaginosis No Yes | 26 6 | 30 12 | 54 17 | 1 2 | 2.13 | 0.7–5.8 | 0.328 |
ORmh: Mantel Haenszel adjusted odds ratio; CI: confidence interval.
Table IV indicates the major independent risk factors of VVS: nulli-pregnant women had a 9.4 times higher risk than women who had been pregnant. OR was 3.8 for bacterial vaginosis, p=0.02, indicating that women reporting treatment for BV had a 3.8 higher risk of vestibulitis than women not having been treated for this condition. Also younger age <26 years was highly associated with VVS OR=13.6, p=0.0001. Current OC did not remain a risk factor, nor did frequent treatment for vulvo-vaginal candidiasis.
Table IV. Independent risk factors for vulvar vestibulitis, using the multivariate logistic model
| Variables | Level | OR | 95% CI | p-value |
| Age < 26 years | Yes/No | 13.5 | 3.0–27.7 | 0.0001 |
| Bacterial vaginosis | Yes/No | 3.8 | 1.1–12.4 | 0.026 |
| Never pregnant | Yes/No | 9.1 | 3.0–27.7 | 0.0001 |
| OR: Odds ratio; CI: confidence interval. |
DISCUSSION
The Norwegian national registration provides an advantage for case-control studies, as a random selection of population-based controls can be performed, and selection bias minimized. Our response rate was relatively low (61%), but as the study protocol guaranteed anonymity for controls towards investigators, we could not use telephone interviews in order to elicit more responses. Fortunately, age and residence in Oslo did not differ between respondents and non-respondents among the controls. Furthermore, we excluded participants reporting entry dyspareunia, in order to analyse only for healthy controls. However, power was reduced, as we expected a response rate of 80% in the controls. The de facto prevalence of current entry dyspareunia was 22% in the control group, for the same effect OR = 3 and type I error of 5%, we would have needed 26 cases and 104 controls to attain a power of 70%. Thus, the real power of our study was over 70%.
Differential misclassification is a concern in any case-control study, as information may be gathered differently for cases and controls. Our controls received a self-administered postal questionnaire addressing the same topics as in the CRF, but were not interviewed. Furthermore, it is probably that cases have a more vivid memory of factors of possible importance to their condition. These information biases – differential misclassification of exposure, and a recall bias – may influence our estimated ORs in over- or under-estimation.
Confounding can be dealt with in various ways at the design stage and in the analysis. When matching is performed, the characteristics chosen for matching are generally those that are known to be strong confounders. All case-control studies on VVS we have found are age-matched (8–14), with little discussion of methodology. We choose not to age-match, as matching does not control for confounders in a case-control study, and thus the influence of the matched factor on the disease cannot be studied (18–20). As expected, age was the major confounder in our study, and was adjusted for in the statistical analyses, through age stratification and statistical modelling.
Coitarche and oral contraception
Age at first intercourse, coitarche, is lower among cases than controls. The difference is not statistically different, and we have not investigated the potential clinical relevance. However, having regular sexual intercourse before the age of 16 years, and using oral contraception for more than 2 years were independent variables increasing the risk of vulvar pain among young girls visiting youth health centres in Stockholm, in a study by Berglund et al. (21) An elaborate case-control study on vestibulitis and OC was performed by Bouchard et al. (11) in 2002, and it was found that when use of OC was started before age 16 years, the risk of vestibulitis was strongly increased: OR 9.3 (CI 3.2–27.2). The risk was increased with the duration of use of oral contraception, and when the brand used was of high progestogenic, high androgenic and low oestrogenic potency. However, and in accordance with the study by Smith et al. from 2002 (13), we did not find use of oral contraception to be a risk factor for VVS. Our ORc of 2.94 was diluted when risk factors were adjusted for age. However, we did not investigate for brands, and it may be worth mentioning that desogestrel-ethinylestradiol (Marvelon®) is seldom used in Norway.
Pregnancy and parity
Our finding that nulli-pregnancy is a characteristic for vestibulitis is in accordance with the findings by Smith et al. (13), who reported nulli-pregnancy to be an independent risk factor for VVS, relative risk 3.3 (CI 1.4–7.6). Reasons for nulli-pregnancy are lifestyle, level of sexual activity, and use of contraception. Whether ever-pregnancy is a true protective factor among nulli-para remains to be investigated further.
Bacterial vaginosis
Treatment for BV was reported by 30% of our cases, and was an independent risk factor, weaker, but in accordance with two other studies: Sarma et al. (12) reported 42.9% of 28 VVS cases to have been treated for BV, Smith et al. (13) 11.6% of 69 cases. OR was 22.2 (2.8–177.2) and 9.4 (1.1–79), respectively. However, vulvar pain might be misattributed to BV (and other conditions) by patients and physicians. The established method for a rapid clinical diagnosis of BV is based on the microscopic evaluation of a wet smear, according to Amsel’s criteria (22). However, patients may be treated for BV without a proper diagnosis, and consequently, there is a risk for a misclassification. But is it possible that BV with its characteristic high pH in vaginal secretions be a true trigger factor for VVS? The discussed correlation between BV and pre-term delivery shows that there is much more to BV than a foul-smelling discharge (23), and the cytokine levels of IL-1alpha and IL-1beta in both cervix and vagina are increased in BV (24–26). Thus, both BV and more subtle changes in the vulvo-vaginal microbiota may be of importance in the pathophysiology of VVS, as well as hormonally induced changes in the vulvo-vaginal mucosa. These “environmental factors” might interact to sensitize the nerve endings of the vestibule. Clinical studies including up-to-date microbiological investigations should be pursued.
In conclusion, it is general knowledge that risk factors found in a case-control study are not equal to causality. However, the causes of vulvar vestibulitis remain unclear, and further investigation of low-grade inflammation of the vagina and vestibulum may provide important knowledge of the aetiology of VVS. Furthermore, proper diagnosis of vulvo-vaginal conditions, and cautious use of antifungal agents and antibiotics, may contribute to a decreased risk of longstanding entry dyspareunia and vulvar vestibulitis in young women with vulvar symptoms, wherever they present for medical attention.
REFERENCES
1. Friedrich EG Jr. Vulvar vestibulitis syndrome. J Reprod Med 1987; 32: 110–114.
2. Danielsson I, Sjöberg I, Stenlund H, Wikman M. Prevalence and incidence of prolonged and severe dyspareunia in women: results from a population study. Scand J Public Health 2003; 31: 113–118.
3. Lundqvist EN, Hofer PA, Olofsson JU, Sjöberg I. Is vulvar vestibulitis an inflammatory condition? A comparison of histological findings in affected and healthy women. Acta Derm Venereol 1997; 77: 319–322.
4. Bohm-Starke N, Hilliges M, Brodda-Jansen G, Rylander E, Torebjork E. Psychophysical evidence of nociceptor sensitization in vulvar vestibulitis syndrome. Pain 2001; 94: 177–183.
5. Bohm-Starke N, Falconer C, Rylander E, Hilliges M. The expression of cyclooxygenase 2 and inducible nitric oxide synthase indicates no active inflammation in vulvar vestibulits. Acta Obstet Gynecol Scand 2001; 80: 638–644.
6. Edwards L, Lynch PJ. The terminology and classification of vulvodynia: past, present and future. The International Society for the Study of Vulvovaginal Disease. Available from: www.issvd [accessed 15 December 2004].
7. Bachmann GA, Rosen R, Pinn VW, Utian WH, Ayers C, Basson R et al. Vulvodynia, a state-of-the-art consensus on definitions, diagnosis and management. J Reprod Med 2006; 51: 447–456.
8. Danielsson I, Eisemann M, Sjöberg I, Wikman M. Vulvar vestibulitis: a multi-factorial condition. Br J Obstet Gynaecol 2001; 108: 456–461.
9. Nylander Lundqvist E, Bergdahl J. Vulvar vestibulitis: evidence of depression and state anxiety in patients and partners. Acta Derm Venereol 2003; 83: 369–373.
10. Sjöberg I, Nylander Lundqvist EN. Vulvar vestibulitis in the north of Sweden. An epidemiologic case-control study. J Reprod Med 1997; 42: 166–168.
11. Bouchard C, Brisson J, Fortier M, Blanchette C, Meisels A. Use of oral contraceptive pills and vulvar vestibulitis: a case-control study. Am J Epidemiol 2002; 156: 254–261.
12. Sarma AV, Foxman B, Bayrili B, Haefner H, Sobel JD. Epidemiology of vulvar vestibulitis syndrome: an exploratory case-control study. Sex Transm Inf 1999; 7: 320–326.
13. Smith EM, Ritchie JM, Galask R, Pugh EE, Jia J, Ricks-McGillan J. Case-control study of vulvar vestibulitis risk associated with genital infections. Infect Dis Obstet Gynecol 2002; 10: 193–202.
14. Bazin S, Bouchard C, Brisson J, Morin C, Meisels A, Fortier M. Vulvar vestibulitis syndrome: an exploratory case-control study. Obstet Gynecol 1994; 83: 47–50.
15. Bergeron C, Moyal-Barracco M, Pelisse M, Lewin P. Vulvar vestibulitis: lack of evidence for a human papillomavirus etiology. J Reprod Med 1994; 39: 936–938.
16. Edgardh K, Abdelnoor M. Longstanding vulval problems and entry dyspareunia among STD-clinic visitors in Oslo – results from a cross-sectional study. Int J STD & AIDS, 2003; 14: 796–799.
17. Bjornerem A, Aghajani E, Maltau JM, Moi H. Occurrence of bacterial vaginosis among abortion seekers. Tidsskr Nor Laegeforen 1997: 10; 117: 1282–1284 [in Norwegian].
18. Kleinbaum DG, Kupper LL, Morgenstern H. Epidemiologic Research. Principles and quantitative methods. New York: Van Nostrand Reinhold, 1982.
19. Rothman KJ, editor. Modern epidemiology. Boston: Little, Brown and Co, 1986.
20. Schlesselman JJ, editor. Case control studies. Oxford: Oxford University Press Inc., 1982.
21. Berglund AL, Nigaard L, Rylander E. Vulvar pain, sexual behavior and genital infections in a young population: a pilot study. Acta Obstet Gynecol Scand 2002; 81: 738–742.
22. Amsel R, Totten PA, Spiegel CA, Chen KC, Eschenbach D, Holmes KK. Non-specific vaginitis. Diagnostic criteria and microbial and epidemiologic associations. Am J Med 1983; 74: 14–22.
23. Donders GG, Van Bulck B, Caudron J, Londers L, Vereecken A, Spitz B. Relationship of bacterial vaginosis and mycoplasmas to the risk of spontaneous abortion. Am J Obstet Gynecol 2000; 183: 431–437.
24. Draper DL, Landers DV, Krohn MA, Hillier SL, Wiesenfeld HC, Heine RP. Levels of vaginal secretory leukocyte protease inhibitor are decreased in women with lower reproductive tract infections. Am J Obstet Gynecol 2000; 183: 1243–1248.
25. Cauci S, Guaschino S, De Aloysio D, Driussi S, De Santo D, Penacchioni P, et al. Interrelationships of interleukin-8 with interleukin-1beta and neutrophils in vaginal fluid of healthy and bacterial vaginosis positive women. Mol Hum Reprod 2003; 9: 53–58.
26. Mattsby-Baltzer I, Platz-Christensen JJ, Hosseini N, Rosen P. IL-1beta, IL-6, TNFalpha, fetal fibronectin, and endotoxin in the lower genital tract of pregnant women with bacterial vaginosis. Acta Obstet Gynecol Scand 1998; 77: 701–706.