Makoto Sugaya and Kunihiko Tamaki
Department of Dermatology, University of Tokyo, 7-3-1, Hongo, Bunkyo-ku, 113-8655 Tokyo, Japan. E-mail: sugayam-der@h.u-tokyo.ac.jp
Accepted January 29, 2007.



Makoto Sugaya and Kunihiko Tamaki
Department of Dermatology, University of Tokyo, 7-3-1, Hongo, Bunkyo-ku, 113-8655 Tokyo, Japan. E-mail: sugayam-der@h.u-tokyo.ac.jp
Accepted January 29, 2007.
Sir,
Nodular fasciitis is a benign lesion arising in the subcutaneous tissue, skeletal muscles and fascia (1, 2). It is important not to confuse the disease with true sarcoma or other malignant tumours. Intravascular fasciitis, which was originally described by Patchefsky & Enzinger (3), is an unusual variant of nodular fasciitis. Only a few cases have been reported in the literature (4–11). Here we report intravascular fasciitis involving the medial border of the foot of a 66-year-old man.
CASE REPORT
A 66-year-old Japanese man was referred to our hospital with a slowly growing subcutaneous nodule on the medial border of the right foot. The lesion was first noticed about 1 year before, with no preceding trauma. The patient had undergone partial gastrectomy for gastric carcinoma a few months before he noticed the lesion. Examination of the lesion revealed a freely mobile non-tender subcutaneous nodule measuring about 10×3 mm. Laboratory data were within normal limits. A simple resection was undertaken.
Histopathological examination showed well-demarcated nodules of spindle-shaped cells within a myxoid stroma in the lower dermis (Fig. 1a). The nodules involved vessel-like structures with surrounding fibrosis. The overlying epidermis and the upper dermis were uninvolved. The spindle-shaped cells were slightly basophilic with ovoid nuclei (Fig. 1b). Mitotic figures were scarcely seen and there was no nuclear atypia. Slit-like capillaries were occasionally seen. No other types of cells, such as lymphocytes or giant cells, were infiltrated. Immunohistochemical studies showed that the spindle cells were positive for vimentin, but negative for desmin, smooth muscle actin, S-100, c-kit, CD31, CD34, von Willebrand factor, carcinoembryonic antigen (CEA) and cytokeratin. Elastica van Gieson staining showed fragmented elastic fibres lining vessel-like structures, suggesting that the spindle cells proliferated within and around blood vessels (Fig. 2).
Fig. 1. (a) Well-demarcated nodules of spindle-shaped cells within a myxoid stroma in the lower dermis (haematoxylin and eosin (H&E) ×40). (b) Basophilic spindle-shaped cells proliferating within and around vessel-like structures (H&E ×400).
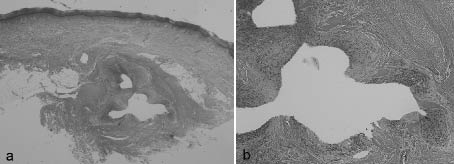
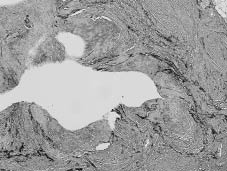
Fig. 2. Elastica van Gieson staining. Fragmented elastic fibres lining vessel-like structure (H&E ×400).
DISCUSSION
Intravascular fasciitis is an unusual variant of nodular fasciitis (3). Its occurrence has been reported in several sites, including small veins and arteries of the limbs and trunk, as well as of the head and neck region. Only a few cases involving the foot have been reported (3, 4). The size of the involved vessels varies from intradermal small veins to large subcutaneous vessels. Extravascular nodular fasciitis often concurred with the intravascular lesions, either as a multi-centricity of the lesion or as a direct extension of the extravascular fasciitis into adjacent vascular structure. In either instance, vascular involvement can be overlooked unless elastic staining is performed to demonstrate the effaced vascular structure. The reported incidence of intravascular fasciitis among nodular fasciitis is rare (12). Compared with ordinary nodular fasciitis, intravascular fasciitis was originally reported to affect the younger population (3). The nodule is usually painless, which was true in this case. The clinical behaviour of this lesion is virtually benign, yet a few cases have been reported to recur after excision (3).
Immunohistochemical characterization has suggested that the proliferative cells in intravascular fasciitis are of myofibroblastic phenotype, as defined by both vimentin and α-smooth muscle actin expression, but lack desmin and CD34 expression, whereas the latter two markers are often observed in angiomyofibroblastic neoplasms of soft parts. In this reported case, spindle cells were negative for smooth muscle actin, but a similar case has been reported previously (6). Due to rich cellularity and mitotic activity, intravascular fasciitis could be confused with other intravascular lesions or malignant tumours. The differential diagnosis includes benign fibrous histiocytoma, pyogenic granuloma, peripheral nerve tumours, spindle cell carcinoma, spindle cell melanoma, myxoid liposarcoma, fibrosarcoma and leiomyosarcoma. The lesion of intravascular fasciitis is usually well defined and spindle cells proliferate with a regular storiform growth pattern. The overlying epidermis is usually unchanged. In addition, some diseases mentioned above can be ruled out by immunohistochemistry. It is of great importance that a diagnosis of intravascular fasciitis is considered and appropriate differential markers are examined.
The aetiology of intravascular fasciitis remains unclear. It is assumed that myofibroblasts within the vessel may give rise to local proliferative changes without any underlying vascular disease (3). Although trauma has been implicated, very few patients give such a history. There was no history of trauma in our case. Preceding thrombosis remains controversial as a possible cause of intravascular fasciitis (11). In our case, fibrous thickening around the vessel and fragmentation of the internal elastic lamina were observed, which are often associated with organizing thrombus. In addition, the patient had undergone partial gastrectomy only a few months previously, which is a risk factor for venous thrombosis. In conclusion, our case suggested the possible involvement of thrombosis in the pathogenesis of intravascular fasciitis.
REFERENCES
1. Konwaler BE, Keasbey L, Kaplan L. Subcutaneous pseudosarcomatous fibromatosis (fasciitis). Am J Clin Pathol 1955; 25: 241–252.
2. Price EB Jr., Silliphant WM, Shuman R. Nodular fasciitis: a clinicopathologic analysis of 65 cases. Am J Clin Pathol 1961; 35: 122–136.
3. Patchefsky AS, Enzinger FM. Intravascular fasciitis: a report of 17 cases. Am J Surg Pathol 1981; 5: 29–36.
4. Sticha RS, Deacon JS, Wertheimer SJ, Danforth RD Jr. Intravascular fasciitis in the foot. J Foot Ankle Surg 1997; 36: 95–99.
5. Samaratunga H, Searle J, O’Loughlin B. Intravascular fasciitis: a case report and review of the literature. Pathology 1996; 28: 8–11.
6. Beer K, Katz S, Medenica M. Intravascular fasciitis. Int J Dermatol 1996; 35: 147–148.
7. Price SK, Kahn LB, Saxe N. Dermal and intravascular fasciitis. Unusual variants of nodular fasciitis. Am J Dermatopathol 1993; 15: 539–543.
8. Kahn MA, Weathers DR, Johnson DM. Intravascular fasciitis: a case report of an intraoral location. J Oral Pathol 1987; 16: 303–306.
9. Freedman PD, Lumerman H. Intravascular fasciitis: report of two cases and review of the literature. Oral Surg Oral Med Oral Pathol 1986; 62: 549–554.
10. Batsakis JG, el-Naggar AK. Pseudosarcomatous proliferative lesions of soft tissues. Ann Otol Rhinol Laryngol 1994; 103: 578–582.
11. Ito M, Matsunaga K, Sano K, Sakaguchi N, Hotchi M. Intravascular fasciitis of the forearm vein: a case report with immunohistochemical characterization. Pathol Int 1999; 49: 175–179.
12. Samaratunga H, Searle J, O’Loughlin B. Nodular fasciitis and related pseudosarcomatous lesions of soft tissues. Aust N Z J Surg 1996; 66: 22–25.

