Sir,
The first published case of a Cryptococcus infection was reported by Zenker in 1861 (1), when he described a case of a man dying from a fungal infection involving the central nervous system (CNS). Thereafter, reports of Cryptococcus infections increased significantly. Today most cases occur in immunocompromised, often HIV-infected, individuals (2).
C. neoformans (CN) is a ubiquitous yeast-like fungus with a highly resistant capsule (3). It is found mainly in the excrement of pigeons, which do not themselves become infected. The most frequent means of acquiring cryptococcosis is by inhalation of contaminated dust particles. The infection may be symptomless and remain unnoticed or may manifest in an atypical pneumonia. An associated disease is chronic meningitis due to a biased predilection of CN for the CNS (4). Other organs, such as lymph nodes, liver, spleen, eyes, and bones, may also become involved. Primary cutaneous infections are extremely rare, especially in immunocompetent individuals.
We describe here a rare pyoderma gangraenosum-like lesion, which was diagnosed as a CN infection. Although the 66-year-old patient was immunocompromised, only a primary cutaneous infection could be verified.
Case report
A 66-year-old hobby pigeon-breeder presented with a tumour, which had been increasing in size for 5 months, on the dorsum of the right wrist following a trauma that had occurred while cleaning the cages (Fig 1a).
The patient had had vitiligo since 2000 and systemic lupus erythematosus since 1996, which was being treated with 5 mg prednisolone daily.
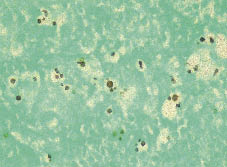
Clinical examination and initial routine investigations, such as abdominal sonography and computed tomography (CT), syphilis-, hepatitis- as well as HIV-serologies, revealed no abnormalities. The only pathological findings were elevated liver transaminases and elevated C-reactive protein. The skin biopsy showed an inflammatory granulomatous reaction of the dermis and upper subcutis, with numerous neutrophil and few eosinophil granulocytes. PAS and Grocott staining revealed capsuled spores (Fig. 2) and hyphae in the upper dermis. Microbiological culture verified a diagnosis of C. neoformans serotype AD, but no antigen could be found in blood samples. The Institute of Hygienics (Robert Koch Institute, Berlin) identified CN subgroup AD in the patient’s pigeonry, i.e. a different one from the one found on the patient. After treatment with itraconazole, 400 mg per day for 2 weeks, followed by a reduction to 200 mg per day for 10 weeks due to elevated liver transaminases, there was a gradual decrease in tumour size and only residual hypopigmentation remained (Fig. 1b).
Fig. 1. (a) Exophytic crustaceous tumour on right hand. (b) After 12 weeks of treatment with itraconazole.
Fig. 2. Grocott staining showing spores (×400).
Discussion
In 1928 Buschke & Joseph (5) were the first to describe primary cutaneous infection with CN and distinguish it from cutaneous manifestation of the systemic infection. Primary cutaneous cryptococcosis with no systemic involvement has rarely been reported, and some authors question its existence (6).
Very few cutaneous infections of CN in immunocompetent patients could be found in the literature (7), with a slightly higher prevalence of male individuals of advanced age. Much more common is the association with organ transplantation or immunosuppressive diseases such as autoimmunodermatoses, tumours and HIV, where cryptococcosis is listed as an AIDS-defining disease.
Our patient showed immunodysregulation caused by an autoimmune disease (systemic lupus erythematosus) and its therapy (prednisolone 5 mg daily for 5 years). The case described here is typical; the patient is a passionate pigeon breeder and reported an injury of his hand, whereafter the skin lesion developed.
The clinical appearance of cutaneous cryptococcosis varies. Papules, nodules and ulcerations, unspecific subcutaneous swellings, abscesses and pustules have been described, giving rise to a number of differential diagnoses, such as pyoderma gangraenosum, erysipeloid, atypical mycobacteriosis, sporotrichosis and neoplasia-like basal cell carcinoma. The notable feature of our case was the pyoderma gangraenosum. A similar case was published in 1981 (8).
Diagnostic strategies should include direct proof of the pathogen by microscopy of infected tissues (e.g. cerebrospinal fluid) or histological samples, as well as by microbiological culture. It is essential to exclude systemic involvement, by carrying out serological examination using latex agglutination tests, which must be repeated in the course of the disease, because sometimes the skin lesions precede infection of the inner organs (7, 9). Chest X-rays are useful for detecting lung infection, but will not lead to a definitive diagnosis of cryptococcosis without the above-mentioned techniques.
Three varieties and five serotypes of CN have been defined (10). In our case, C. neoformans serotype AD was found in the lesion, although only CN var. grubii could be identified in the pigeonry. Maybe the pigeons introduced the other serotype to their pigeonry and the patient was less tolerant to this subgroup.
Azoles are the first choice of treatment for cryptococcosis, and these are relatively well tolerated (11).
It is crucial to distinguish involvement of the CNS, when fluconazole should be used; because of a low protein bond this drug can penetrate the blood–brain barrier more easily. Unfortunately, it is less effective than amphotericin B in treating severe forms of meningitis.
A literature review showed no consensus regarding doses of drugs or duration of treatment. Common dosages are approximately 100–400 mg/day azoles, but in the case of meningitis up to 800 mg/day fluconazole could be used for 1–6 months.
Typical side-effects of azoles are gastrointestinal and allergic reactions, as well as the elevation of liver transaminases as described here, which may lead to dosage reduction.
Other undesirable side-effects are inhibition of steroid synthesis and associated symptoms such as menstrual disorders, impotence and gynaecomastia. Amphotericin B is very toxic. Side-effects such as fever, shaking chills and gastrointestinal disorders are typical. The most severe risk is its nephrotoxicity.
Prevention of exposure to the ubiquitous pathogen CN is only possible by wearing protective gloves and respirator masks. In the case of systemic infection and immunosuppression, hobbies such as pigeon breeding or gardening must be abandoned, but in local infections, such as the case presented here, it may be safe to continue these activities if protective measures are strictly adhered to.
REFERENCES
1. Zenker FA. Encephalitis mit Pilzentwicklungen im Gehirn. Jahresb. D Gesellsch. F Nat U Heik in Dresd 1861; 62: 51.
2. Chaudhary NW, Sardane K, Kumar P, Dewan V, Anand VK. Disseminated infection with cryptococcus neoformans var neoformans in an 8 years immunocompetent girl. Indian J Pediatr 2005; 72: 85.
3. Bose I, Reese AJ, Ory JJ, Janbon G, Doering TL. A yeast undercover: the capsule of cryptococcus neoformans. Eukaryotic Cell 2003; 2: 655–663.
4. Carton CA, Mount KA. Neurosurgical aspect of cryptococcosis. J Neuro Surg 1951; 8: 143.
5. Buschke A, Joseph A. Blastomycosis. In: Jadassohn, J, editor. Handbuch der Haut und Geschlechtskrankheiten. Voll II, Berlin: Springer-Verlag, 1928.
6. Sarosi GA, Silberfarb PM, Tosh FE. Cutaneous cryptococcosis: a sentinel of disseminated disease. Arch Dermatol 1971; 104: 1–3.
7. Quéreux G, Milpied B, Morin O, Andrès P, Parant E, Poirier P, et al. Cryptococcoses cutanèes primitives chez des sujets sèronègatifs pour le VIH. Ann Dermatol Venereol 2000; 128: 1009–1013.
8. Massa MC, Doyle JA. Cutaneous cryptococcosis simulating pyoderma gangrenosum. J Am Acad Dermatol 1981; 5: 32–36.
9. Christianson JC, Engber W, Andes D. Primary cutaneous cryptococcosis in immunocompetent and immunocompromised hosts. Med Mycol 2003; 41: 177–188.
10. Enache-Angoulvant A, Chandenier J, Symoens F, Lacube P, Bolognini J, Douchet C, et al. Molecular identification of Cryptococcus neoformans serotypes. J Clin Microbiol. 2007; 45: 1261–1265.
11. Feldman SR, Fleischer AB. Fluconazole treatment of cutaneous cryptococcosis. Arch Dermatol 1992; 128: 1045–1046.