Marta Carlesimo1, Laura Fidanza1, Elena Mari1*, Guglielmo Pranteda1, Claudio Cacchi2, Barbara Veggia3, Maria Cristina Cox1 and Germana Camplone1
1UOC Dermatology, 2UOC Histopathology and 3UOC Haematolohy, II Unit University of Rome Sapienza Via di Grottarossa, 1039, IT-00189 Rome, Italy. *E-mail: elenamari4@virgilio.it
Accepted September 25, 2008.
Sir,
Figurate erythemas are classified as erythema annulare centrifugum (EAC), erythema gyratum repens, erythema migrans and necrolytic migratory erythema. Differential diagnoses are mycosis fungoides, urticaria, granuloma annulare and pseudolymphoma.
EAC consists of recurrent and persistent erythematous eruptions or urticarial papules forming annular or serpentiginous patterns with an advancing macular or raised border and scaling on the inner aspect of the border.
EAC was first described by Darier in 1916, and classified in 1978 by Ackerman into a superficial and a deep type (1, 2). EAC can be associated with a wide variety of triggers including infections, food and drug ingestion, endocrinological conditions and as a paraneoplastic sign. A diagnosis of EAC should be followed by diagnostic work-up because it may result in the discovery of an underlying disease. We describe here a 68-year-old man affected by EAC who developed small B-cell non-Hodgkin’s lymphoma 7 years later.
CASE REPORT
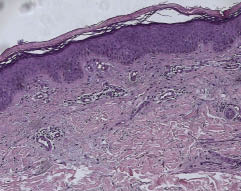
In October 2006, a 68-year-old man presented with EAC on his trunk and extremities (Fig. 1). EAC had occurred 6 years before, as determined by skin biopsy. A new skin biopsy confirmed the diagnosis EAC of superficial type (Fig. 2). Previous investigations were normal, but as the lesions persisted further investigations were carried out. Hepatic, pancreatic, renal function and blood pictures were normal. The lymph nodes on the left side of his neck were approximately 4.5 cm in diameter.
Fig. 1. Erythemato-infiltrated annular lesions on legs.
Fig. 2. Skin biopsy: papillomatosis, hyperkeratosis parakeratosis, perivascular infiltrate of lymphocytes confined to the superficial dermis and fragmentation of elastic fibers.
A lymph node biopsy revealed a small B-cell non-Hodgkin’s lymphoma. The neoplastic cells were positive for CD20/79a and cyclin d1. A bone marrow investigation showed scattered CD20/79a-positive lymphocytes. GeneScan analysis and heteroduplex on polyacrylamide gel analysis showed a monoclonal B lymphocyte population.
DISCUSSION
EAC is a figurate erythema of unknown aetiology. It has been associated with many different entities, including infections (bacterial, viral, parasitic or fungal), food allergy and drug reactions (spironolactone, amitryptiline, ampicillin, cimetidine, hydrochlorothiazide, salicylates), haematological conditions (polycythemia vera, cryoglobulinaemia, myelodysplastic syndrome, hypereosinophilic syndrome), endocrinological conditions (hyperthyroidism, Hashimoto thyroidities, autoimmune progesterone dermatitis), hepatic diseases and malignant neoplasms (3, 4). Malignant diseases associated with EAC include myelomatosis, Hodgkin’s lymphoma, acute leukaemia, prostatic adenocarcinoma, nasopharyngeal carcinoma and histiocytosis. The relationship with non-Hodgkin lymphoma is rare. EAC appears equally in female and male patients and at any age.
There are two types of EAC: a deep type with indurated borders, without desquamation and rarely itching. There is a lymphocytic infiltration in the mid and deep dermis. A superficial type with desquamation following the advancing border and itching is more frequent. Epidermal changes, such as focal epidermal spongiosis and focal parakeratosis, and perivascular lymphocytic infiltrate are present (4, 5).
It is not clear whether these represent two separate diseases or a continuous range. In fact, clinically it has been stated that the superficial variant differs only by the presence of a delicate annular rim of scale that trails behind the advancing edge of erythema. EAC is characterized by slowly migrating, recurrent, annular erythematous eruptions. It can begin as a single lesion or as multiple erythematous lesions with urticaria-like papules that enlarge by peripheral extension to form round arcuate or polycyclic figures with central clearing. Lesions tend to appear on the trunk, proximal parts of the extremities and, more frequently, in the superficial type appear especially on the buttocks (3, 5).
EAC is currently considered to be a distinctive hypersensitivity reaction that may be triggered by many different antigens and disappears after 1–2 weeks.
The skin eruption may be the presenting sign of an underlying disease. In the case described here cutaneous lesions of EAC were not responsive to topical steroid therapy but only after chemotherapy (5, 6).
Only one published case was found of EAC persisting for 2 years associated with non-Hodgkin’s lymphoma (5). We therefore want to emphasize that EAC can appear many years before the onset of lymphoma.
In conclusion, a diagnosis of EAC should lead to considerations of an underlying disease.
REFERENCES
1. Darier J. Erytheme annulaire centrifuge (erytheme papulo-circine migrateur et cronique) et de quelques eruptions analogues. Am Dermatol Sylp 1916; 6: 57–76.
2. Weyers W, Diaz-Cascajo C, Weyers I. Erythema annulare centrifugum: results of a clinicopathologic study of 73 patients. Am Dermatol 2003; 25: 451–462.
3. Weyers W, Diaz-Cascajo C, Weyers I. Erythema annulare centrifugum. Am J Dermatopathol 2003; 25: 451–462.
4. Sigal-Nahum M, Cornelis F, Gaulier A, Konqui A, Pulik M, Sigal S. Erytheme annulaire centrifuge et lymphome non Hodgkinien. Ann Dermatol Venereol 1987; 114: 1445–1447.
5. Ural AU, Ozcan A, Avcu F, Kaptan K, Tastan B, Beyan G, Yalcin A. Erythema annulare centrifugum as the presenting sign of CD 30 positive anaplastic large cell lymphoma-association with disease activity. Haematologia 2001; 31: 81–84.
6. Tuzun Y, Antonov M. Figurate erythemas. J Turk Acad Dermatol 2007; 1: 2.