Tamihiro Kawakami, Takeshi Kawanabe and Yoshinao Soma
Department of Dermatology, St Marianna University School of Medicine, 2-16-1 Sugao, Miyamae-ku, Kawasaki, Kanagawa 216-8511, Japan.
E-mail: tami@marianna-u.ac.jp
Accepted January 9, 2009.



Tamihiro Kawakami, Takeshi Kawanabe and Yoshinao Soma
Department of Dermatology, St Marianna University School of Medicine, 2-16-1 Sugao, Miyamae-ku, Kawasaki, Kanagawa 216-8511, Japan.
E-mail: tami@marianna-u.ac.jp
Accepted January 9, 2009.
Sir,
Chronic myeloid leukaemia (CMV) is a clonal myeloproliferative disorder, in which the Philadelphia chromosome is the cytogenetic hallmark. It is characterized by the t(9;22) translocation, which in turn creates the chimeric bcr-abl oncogene coding for a constitutively activated tyrosine kinase (1, 2). Imatinib mesylate is a tyrosine kinase inhibitor that targets the bcr-abl protein, c-kit, and platelet-derived growth factor receptors and is used to treat CMV, gastrointestinal stromal tumours, and dermatofibrosarcoma protuberans (3, 4). The development of the specific inhibitor of bcr-abl tyrosine kinase is a notable success in the treatment of CMV and has recently been approved as a first-line treatment for CMV (5). Adverse cutaneous reactions to imatinib mesylate are not infrequent, but their clinical and histopathological features have generally been poorly characterized. We report here a Japanese patient with cutaneous lichenoid eruptions that occurred during imatinib mesylate treatment for CMV.
CASE REPORT
In June 2005, a 53-year-old Japanese man was diagnosed with CMV and treatment with imatinib mesylate (Gleevec®; Novartis, Tokyo, Japan) was commenced at a daily dose of 400 mg. The patient was not taking any other drugs. Two months later, generalized violaceous,
mildly pruritic papules and plaques appeared on the patient’s abdomen and proximal upper extremities (Fig. 1). The skin lesions subsequently expanded
gradually in a symmetrical fashion to the trunk and upper extremities and infiltrated those regions. A skin biopsy from the trunk demonstrated vacuolar degeneration of the basal layer, as well as band-like dense lymphocytic infiltrations, pigmentary incontinence, and oedema in the upper dermis (Fig. 2). A diagnosis of cutaneous lichenoid drug eruption
associated with imatinib mesylate was made based on the clinical and histopathological findings, which were highly consistent with lichen planus. There was also a strong correlation between the time course of the reaction and the administration of imatinib mesylate. However, imatinib mesylate was deemed an appropriate treatment in this case of CMV, and therefore was continued. The daily dose of imatinib mesylate was decreased to 200 mg and topical corticosteroids were administered, leading to a partial improvement in the skin manifestations. One year later, after the dose was increased to 400 mg/day to treat an acute aggravation of the CMV, there was a re-emergence of the skin eruption. Coinciding with this increased
dosage, the patient developed an erythematous
cutaneous eruption with lichenoid papules on the trunk and upper extremities. No other non-haematological side-effects were observed in this patient.
DISCUSSION
To date, there have been reports of eight patients with cutaneous lichenoid eruption associated with imatinib mesylate treatment for CMV (Table I) (6–9). Of these cases, four (50%) were associated with oral involvement, but this was not the case in our patient. Imatinib mesylate has also been reported to induce lichenoid lesions only in the mouth. The lichenoid drug eruptions were suggested to be dose-related, appearing in all eight patients at doses of imatinib mesylate of 400 mg daily or greater. The time from the start treatment with imatinib mesylate to the onset of eruptions was approximately the same in all patients except one, in whom the appearance of cutaneous lesions occurred approximately 2–3 months after the start of treatment. It is generally believed that imatinib mesylate-induced cutaneous eruptions are related more to pharmacological effects than to a hypersensitivity reaction (10, 11). The cutaneous lichenoid eruptions may be a result of the pharmacological effects of imatinib mesylate, and appear to be dose-dependent.
Based on the findings reported here, we propose that imatinib mesylate be included in the list of drugs that can cause cutaneous lichenoid reactions. Lichenoid drug-induced eruptions can clinically and histologically resemble idiopathic or classic lichen planus. Integrating drug history, clinical morphology, clinical distribution, and histopathology can aid in the differentiation (12). We wish to emphasize the significance of taking a detailed anamnestic history, including drug dosages and interval appearance, in order to make the correct differential diagnosis between lichenoid drug-induced eruptions and lichen planus. As the use of imatinib mesylate for patients with CMV is increasing, clinicians should be aware of the possibility of cutaneous lichenoid eruptions occurring as an adverse effect.
The authors declare no conflict of interest.
REFERENCES

Fig. 1. Examination revealed violaceous macules on (a) the patient’s abdomen and (b) a left axillary lesion.
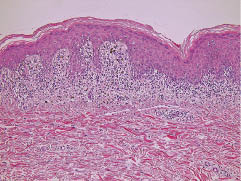
Fig. 2. Histopathological examination revealed apoptotic keratinocytes with vacuolar change and a band of lymphocytic infiltrate in the papillary dermis (haematoxylin-eosin ×100).
Table I. Eight patient reports of cutaneous lichenoid eruption induced by imatinib mesylate treatment of chronic myeloid leukaemia
| Patient | Age (years)/sex | Chronic myeloid leukaemia | Imatinib dose | Interval to appearance | Location of lesions | Mucosal involvement |
| 1 (6) | 52/M | 5 | 400 | 2 months | Face, trunk, extremities | – |
| 2 (7) | 76/M | NA | 300–400 | Few days | Thorax, upper extremities | – |
| 3 (7) | 60/M | NA | 400 | 2 months | Face, wrist, neck, penis, anal | + |
| 4 (7) | 50/F | NA | 400 | 2 months | Face, chest, upper extremities | + |
| 5 (8) | 69/F | 6 | 400 | 2 months | Face, trunk, buttocks, lower extremities | + |
| 6 (8) | 65/F | 3 | 400 | 3 months | Trunk, lower extremities | + |
| 7 (9) | 56/M | 3 | 600 | 2 months | Chest, extremities | – |
| 8 present study | 53/M | 2 months | 400 | 2 months | Trunk, upper extremities | – |
NA: not available.

