Yasutoshi Hida1, Yoshiaki Kubo1*, Yukiko Nishio2, Shinji Murakami2, Daisuke Fukumoto1, Koji Sayama2, Koji Hashimoto2 and Seiji Arase1
Department of Dermatology, 1Institute of Health Biosciences, The University of Tokushima Graduate School, 770-8503 Tokushima, and 2Ehime University School of Medicine, Shitsukawa, Toon, Ehime, Japan. *E-mail: ykubo@clin.med.tokushima-u.ac.jp
Accepted February 26, 2009.
Sir,
Fibroblast growth factor receptor 3 (FGFR3) belongs to the transmembrane tyrosine kinase receptors (1). Constitutive activating FGFR3 germline mutations cause genetic syndromes with acanthosis nigricans (AN) (2–5). In addition to hereditary forms of AN, some sporadic forms are known. Among these, the lesions linked with malignancy are called malignant acanthosis nigricans (MAN), which are more severe and more extensive than other sporadic forms of AN. We describe here two cases of MAN and examine the role of the FGFR3 signalling pathway in MAN.
PATIENTS AND METHODS
Case 1. A 68-year-old Japanese man presented in October 1999 with a 4-month history of darkening and thickening of the skin on his face, neck, axillae, groin, hands and feet. On physical examination he had velvety hyperpigmented plaques on the face (Fig. 1) neck, axillae, groin, and dorsal and palmar aspects of his hands and feet. Soft papillomas and warty nodules studded the affected surface. Thickening and papillation without hyperpigmentation was evident on the lips, gingiva, and hard plate. A skin biopsy specimen taken from his axillae revealed hyperkeratosis and mild acanthosis with dermal papillomatosis. A gastroscopy showed a Borrmann type 4 tumour located in the cardiac part of the stomach, and histological examination revealed a poorly differentiated adenocarcinoma. We diagnosed this case as MAN. He underwent a palliative gastrectomy in November 1999, because the gastric cancer had directly invaded the diaphragm, and his para-aortic lymph nodes were swollen. His skin improved after the operation, but subsequently worsened again with the development of metastatic lesions. He died in April 2000 with peritoneal dissemination.
Fig. 1. Clinical features of malignant acanthosis nigricans. Hyperpigmentation, intensified skin marking, and hypertrophy of the skin were seen.
Case 2. A 70-year-old Japanese man presented in January 2004 with a 4-month history of darkening and thickening of the skin on his face. On physical examination, he had velvety hyperpigmented plaques on the face neck, axillae, and dorsal aspects of his hands. Soft papillomas and warty nodules studded the affected surface. His oral mucosa gradually became diffusely thick, and both palms became diffusely hyperkeratotic. A gastroscopy showed a Borrmann type 1 tumour located in the greater curvature of the stomach, and histological examination revealed a poorly differentiated adenocarcinoma. This case was also diagnosed as MAN. He underwent a total gastrectomy for the proximal gastric cancer in March 2004. He received Tegafur after the operation. His abdominal lesions currently remain in remission 4 years after surgical removal. His skin lesions have been improving since the operation.
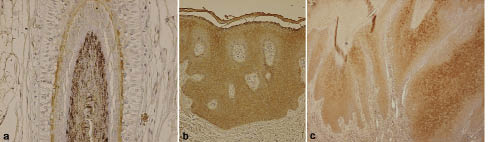
In order to elucidate the pathogenesis of MAN, we examined FGFR3 protein expression in these two cases, compared with 20 samples of normal skin, by immunohistochemical analysis. The source of the normal skin is shown in Table I. Immunohistochemical studies with a mouse monoclonal anti- FGFR3 antibody (B-9: sc-13121, Santa Cruz Biotechnology, Santa Cruz, USA) were performed as described previously (6). FGFR3 protein expression was seen in the cytoplasm and cell membrane, and immunoreactivity for FGFR3 in the internal root sheath of hair follicles was regarded as a positive control (7) (Fig 2a). Results of the immunohistochemistry were summarized in Table I. FGFR3 immunoreactivity in normal epidermis was negative (–) to moderately positive (++) in the suprabasal layer to granular layer. In both MAN cases, the epidermis showed strong expression of FGFR3 (+++; Fig. 2 b–c).
Table I. Summary of the results of fibroblast growth factor receptor 3 (FGFR3) expression
| Lesion | FGFR3 expressiona |
| (–) | (+) | (++) | (+++) | Sum |
| Normal skin | 10 | 8 | 2 | 0 | 20 |
| Face | 3 | 4 | 0 | 0 | 7 |
| Neck | 1 | 1 | 1 | 0 | 3 |
| Axilla | 1 | 0 | 0 | 0 | 1 |
| Trunk | 2 | 3 | 1 | 0 | 6 |
| Arm | 2 | 0 | 0 | 0 | 2 |
| Leg | 1 | 0 | 0 | 0 | 1 |
| MAN | 0 | 0 | 0 | 2 | 2 |
a(–) <5% positive cells; (+) 5–25%; (++) 25–50%; (+++) >50%.
MAN: malignant acanthosis nigricans.
Fig. 2. Immunohistochemical staining for fibroblast growth factor receptor 3 (FGFR3). (a) Typical images of FGFR3 staining in the internal root sheath of a normal hair follicle (positive control, original magnification, × 200). (b–c) FGFR3 staining of skin in malignant acanthosis nigricans (MAN) FGFR3 expression was detected throughout the acanthotic lesion (original magnification, ×100). (b) This sample was taken from axillae of case 1. (c) A verrucous plaque in case 2 (original magnification × 40).
DISCUSSION
Activating FGFR3 germline mutations in hereditary diseases associated with AN induce a proliferative effect on keratinocytes (2–5). Similar mutations were also identified in benign skin lesions, either as embryonic mutations in epidermal naevi or somatic mutations in seborrhoeic keratoses (6, 8–10), both of which share the same histological features as AN. Recently, Hafner et al. (11) reported that the activating mutations of the PI3K3CA gene, which is an important downstream target of the FGFR3 signalling pathway, were detected in epidermal naevi and seborrhoeic keratoses. Furthermore, we revealed that strong expression of FGFR3 was frequently observed in seborrhoeic keratoses by immunohistochemical analysis, and that activation of FGFR3 might be a common feature in tumourigenesis in seborrhoeic keratoses (6).
We speculated that activation of FGFR3 might have some relevance to the formation of MAN, and investigated FGFR3 expression in two cases of MAN and 20 samples of normal epidermis by immunohistochemical analysis. Normal epidermis was weakly positive, and the expression was localized to the suprabasal to granular layers, as previously reported (7). Both cases of MAN tested strongly positive for FGFR3, and the expression spread throughout the acanthotic lesions. These results indicate activation of FGFR3 to have some relevance to the development of MAN, probably due to the proliferative effect on epidermal keratinocytes.
Previous reports suggested that tumour growth factor-α (TGF-α) produced from gastric cancers binds and activates epidermal growth factor receptor (EGFR) on keratinocytes to form the lesions of patients with MAN (12–14). Haase et al. (14) demonstrated that ERK, a mitogen-activated protein kinase (MAPK), was also activated in the lesions of MAN patients, probably as a result of signal transduction via the ras/MAPK pathway through activation of EGFR. The activation of FGFR3 might also contribute to ras/MAPK signalling in the lesions, because EGFR and FGFR3 are both transmembrane tyrosine kinase receptors (TKRs) and located upstream of the ras/MAPK pathway (15). Activation of insulin-like growth factor receptor, which is another TKR, was also shown in insulin-resistant diabetes mellitus with AN (15). FGFR3 may have different physiological effects from EGFR. In contrast to normal epidermis, expression patterns of EGFR and FGFR3 were similar in MAN, with these receptors spread diffusely throughout the acanthotic lesions from the epidermis (14). Further investigations are needed to elucidate how EGFR and FGFR3 cooperate in the development of MAN.
REFERENCES