Bullous pemphigoid is associated with antibodies to a 230 kDa and a 180 kDa protein. In a literature review we investigated the role of auto-antibodies as detected by different serological assays. Nine reports containing data on 143 patients were analyzed. Pre-treatment data showed that indirect immunofluorescence, enzyme-linked immunosorbent assay (ELISA) and immunoblotting offer an 82.2% or greater probability of being positive. At the end of the study period, all patients had clinically improved, whether or not they were on therapy. Auto-antibodies were present in 29% of patients evaluated by monkey esophagus immunofluorescence and 75% of those evaluated by human skin immunofluorescence. Positive titers were also reported in 67.6% of patients evaluated by ELISA. In 100% of patients in whom immunoblotting was performed the titers became negative. In 3 patients (5.3%) using human skin immunofluorescence and in one patient (1.4%) using ELISA the titers were increased at the end of the study period. The correlation between anti-basement membrane zone antibodies and the clinical course of bullous pemphigoid requires further and long-term studies. Key words: anti-basement membrane zone antibodies; remission; indirect immunofluorescence; ELISA; clinical correlation; bullous pemphigoid.
(Accepted November 5, 2009.)
Acta Derm Venereol 2010; 90: 115–121.
A. Razzaque Ahmed, Center for Blistering Diseases, New England Baptist Hospital, 70 Parker Hill Avenue, Suite 208 Boston, MA 02120, USA. E-mail: arahmedmd@msn.com
Bullous pemphigoid (BP) is a chronic subepidermal blistering disease of the skin that mainly affects the elderly, with an annual incidence ranging from 2.6 cases per million population in the Arabian Gulf to 14 cases per million population in north-east Scotland (1–3). Clinically, BP is characterized by large, tense bullous lesions, but may begin as erythematous macules, urticarial papules or plaques (4).
The pathogenesis of BP is characterized by tissue-bound and circulating IgG auto-antibodies against two components of the hemidesmosome of stratified epithelia, referred to as BP 230 kDa (BPAg1) and BP 180 kDa (BPAg2) (5, 6). BPAg1 is a cytoplasmic protein involved in the anchorage of intermediate filaments to the cytoskeleton. BPAg2 is a transmembrane adhesion molecule with several collagenous extracellular domains (7). In the neonatal mouse model, antibodies to BPAg2 appear to be important in subepidermal blister formation in mice (8, 9). BPAg1 may have a secondary role, but its exact functions in the pathogenesis is not fully defined (10, 11).
Schmidt et al. (12) first demonstrated a positive correlation between clinical disease activity and antibodies to BPAg2 as detected by enzyme-linked immunosorbent assay (ELISA). This correlation was similar to that observed between the auto-antibodies to desmogleins in patients with pemphigus vulgaris (13). However, the positive correlation in BP was contrary to earlier observations using the standard indirect immunofluorescence (IIF) assay (14–18). Hence, the role of the antibodies to both BPAg1 and BPAg2 during the clinical course of the disease is not fully understood.
In this review we analyzed the available data with the aim of answering the following questions: (i) What is the range of antibody titres at the beginning of the treatment and when patients are in complete remission on or off therapy, as measured with different assays? (ii) Does the nature of treatment influence the antibody titer at the end of therapy and during follow-up? (iii) Does the severity of the disease correlate with the antibody titers during treatment and follow-up?
MATERIALS AND METHODS
A PubMed search was conducted using the following key words: BP180, BP230, BPAg1, BPAg2, bullous pemphigoid, auto-antibodies titer, disease activity, and clinical outcome. Nine reports, which contained data on 143 patients (12, 16, 17, 19–24), published between August 1977 and February 2009, were included in this analysis. However, 51 studies were excluded because they lacked the inclusion criteria set out below. Moreover, many of these studies had few patients or case reports, and lacked information on antibody titers during the course of the disease. More importantly several studies not included in this review lacked data on treatment and follow-up of patients after treatment was begun. Consequently, the authors felt that the inclusion of patients from the 51 studies would prevent them from conducting the analysis they had intended to do. This has reduced the total number of patients and studies used in this analysis, but has refined the quality and impact of the message of our study.
The studies included in this analysis were based on the following inclusion criteria: (i) English language; (ii) adult patients only with clinical features of BP; (iii) a sub-epidermal blisters with a routine histology; (iv) direct immunofluorescence studies of perilesional skin demonstrating linear deposition of linear IgG and/or C3 on the basement membrane zone (BMZ); (v) when available, on salt-split skin (SSS) analysis binding of auto-antibodies to the roof of the blister; (vi) minimum of five patients in each report; (vii) availability of data of at least one serological antibody assay before beginning systemic therapy and at the end of the study period; (viii) duration of therapy of at least one month; (ix) availability of information on clinical outcomes at the end of the study period.
The following information was obtained from each study: number of patients treated, patients’ demographics, initial systemic treatment, and treatment at the end of the period when available, serological studies that included auto-antibody titer before and at the end of the study period. The serological values were determined by IIF, using monkey esophagus (ME) or normal human skin (NHS) as a substrate, with a standard or SSS technique, and by ELISA and immunoblotting (IB).
For the purpose of this analysis, clinical remission is defined as complete healing of existing lesions (erythema and/or erosions and/or bullae) and the cessation of new blister formation, which may be associated with use of minimal or no systemic therapy. The end of study period is defined as the time at which patients were last examined and evaluated by the individual authors. Serological remission is defined as the total absence of antibodies against the BMZ in the sera of the patient.
RESULTS
The data from nine reports, which included 143 patients, is presented in Table I. All but seven patients (4.89%) with mild diseases required systemic therapy. Specific data about the number of patients on different systemic and/or topical treatments was not available for two reports (17, 24). All patients clinically improved with the treatment(s) they received (12, 16, 17, 19–24). However, eight patients still had mild disease at the end of the study period (5.59%) (12, 20, 22). Seventy-eight (54.5%) of these patients were still receiving systemic therapy, and in 53 (37%) systemic therapy was discontinued at the time of reporting. In 10 patients (6.9%) the authors indicated that the patients were in clinical remission, but did not specify whether these patients were still receiving therapy (19). Twenty patients (13.9 %) developed a recurrence after they stopped systemic therapy or were on minimal maintenance therapy without disease (12, 16, 19, 20, 24). Four patients (2.7%) deliberately stopped their medications (12, 24). Two patients (1.39%) treated with only prednisolone died of a massive gastrointestinal bleeding and a Gram-negative septicemia (16).
Table I. Antibody profiles in patients with bullous pemphigoid during treatment and follow-up
| Ref. | Pat. n | Mean age Race | Sex (M/F) | No. of positive tests (titers) | Total length of therapy (months) | Type of therapy (n) | Patients in CR ON or OFF therapy (n) |
| Type of serology | Prior therapy n [range] n (mean) | Post-therapy n [range] n (mean) |
| Feng et al. (24) | 20 | 68 NA | 11/9 | SSS-IIF ELISABPAg2 | 20 [1:20–1:160] 19 (0.520 OD492) | 13 [0–1:160] 15 (0.215 OD492) | NA | C +/- AZA or CY or T+N | ON (20)1 |
| Tsuji-Abe et al. (23) | 14 | NA | | HS-IIF ELISABPAg2 | 14/ [1:160–1:1280] 11 (52.55) | 14 [1:160–1:13209 Increase in titer in 2 11/ (15.61) (ID) | 12–36 | C (6), C+AZA (2) C+T/N (6) | ON (10) OFF (4) |
| Izumi et al. (22) | 5 | 72.4 A | 1/4 | ELISABPAg2 | 5 [52.7–1374] (ID) | [20.3–161] (ID) | 3 | T (1), C (1), C+T (1), C+D (2) | ON T or C tap. (1) ON C tap, T unch (1) ON C tap, D unch (2) |
| Sami et al. (21) | 10 | 76 Ca | 10/0 | IBBPAg1 IBBPAg2 | 10 (2600) 9 (2380) | 0 (0) 0 (0) | 44 | IVIg + C | OFF (10) |
| Kobayashi et al. (20) | 7 | 63 A | 2/5 | HS-IIF ELISABPAg2 | 6 [0–1:2560] 5 (10–200) (ID) | 6 [0–1:2560] Increase in titer in 1 3/7 (0–40) (ID) Increase in titer in 1 | 12–144 | C (1), C+T/N (3), C+D (1), C +PM (1), C+D+T/N (1) | ON C tap (3) ON C tap, T/N unchanged (3) ON C, dapsone stopped, AZA (1) |
| Amo et al. (19) | 10 | 66.9 NA | 5/5 | ELISABPAg2 | 10 [0.257–1.896) (ID] | 4 [0.008–1.253] (ID) | 3–52 | C (3), C+T (1), C+D (1), C+D+Cy (1), C+Cy+Cycl (1), C+T+D+Cy (1), C+D+Cycl (1), C+T+D+Cy+Cycl (1) | ON or OFF (10) |
| Schmidt et al. (12) | 15 | 69 NA | 7/8 | SSS-IIF ELISABPAg2 | 15 [1:20–1:640] 15 (0.304–1.218) (OD492) | 12 [0–1:320] 10 (0.173–0.864) (OD492) | 2 | C+D (9) T/N+TS (6) | ON (9) OFF (6) |
| Hadi et al. (17) | 26 | 73 NA | 18/33 | ME-IIF | 26 [1:40–1:1280] | 15 [0–1:320] | NA | NA | OFF (26) |
| Ahmed et al. (16) | 36 | 80.8 Ca (34) AA (4) | 16/20 | ME-IIF | Mild 4/7 [1:10–1:640] Moderate 9/12 [1:10–1:1280] Moderate/severe 5/6 [1:10–1:640] Severe 7/11 [1:10–1:5120] | 1/7 NA 2/12 NA 0/6 (0) 0/11 (0) | 19–24 (for all patients) | TS (7) C (14) C+AZA (15) | OFF (7) 2 deaths ON C tap (12) ON C+AZA tap (15) |
1C tapered to half the initial dose.
2Only for 2 representative patients.
CR: complete remission; NA: not available; Ca: Caucasian; A: Azsiatic; AA: African Americans; ID: index value = (patient serum OD – negative control OD)/(positive control OD – negative control OD) × 100; OD492: optical density; tap: tapered; unch: unchanged; IVIg: intravenous immunoglobuline; C: corticosteroids; AZA: azathioprine; T: tetracycline; N: nicotinamide; D: dapsone; CY: cyclophosphamide; Cycl: cyclosporine; PL: plasmapheresis; TS: topical steroids; PM: pulse with methylprednisolone.
Serological analysis using IIF prior to, and at the end of, the study period was performed on 118 patients (82.5%). In 62 patients (52.5%) ME, and in 56 patients (47.4%) NHS was used as substrate. Of these 56 patients, in 42 (75%) SSS IIF studies were performed.
Among the 62 patients whose sera was evaluated by IIF using ME, 51 (82.2%) were positive prior to therapy. In 18 patients (29%) the antibody titers remained positive at the end of the study period (16, 17).
Among the 56 patients whose sera was evaluated by IIF using NHS, 55 (98.2%) were positive prior to therapy. At the end of the study period, 45 (80.3%) continued to remain positive (12, 20, 23, 24), of which in three patients (6.6%) the anti-BMZ antibody titers were increased (20, 23).
Antibodies against BPAg2 were studied in only 71 of the 143 patients (49.6%), using ELISA (rNC16a domain). Among these, in 65 (91.5%) the ELISA levels were positive prior to beginning systemic therapy (12, 19, 20, 22–24). In 48 patients (67.6%) at the end of the study period (12, 19, 20, 22–24) the ELISA was still positive, of which 40 patients (83.4%) were in complete clinical remission and eight patients (16.7%) still had mild disease. The levels of the antibodies to BPAg2 were lower when compared with pre-treatment levels. Among these 48 patients, only one (2.08%) showed an increased mean index value (20). In 23 patients (32.2%) at the end of the study period when no clinical disease was present no antibodies were detected (12, 19, 20, 22–24). In six patients (8.4%) anti-BMZ antibodies as detected by ELISA were negative at the beginning and the end of the study (20, 23, 24).
The duration of the post-therapy follow-up period was provided in five studies in 101 patients (70.6%) and ranged from 7 to 60 months (12, 16, 17, 21, 23).
IB to both antigens BPAg1 and BPAg2 was performed in 10 patients (6.9%) (21). Pre-therapy, nine patients were positive BPAg2 (90%) and all patients were positive to BPAg1. At the end of the study period and during the follow-up, all patients were negative to both BPAg1 and BPAg2. Only one patient’s auto-antibodies to BPAg2 were not detected during the course of the therapy and during the follow-up period after therapy (21).
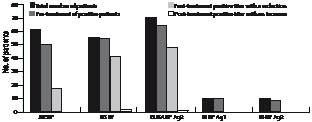
The comparison of serological data using IIF and ELISA on the patients prior to therapy and the end of the study period is presented in Fig. 1. In some patients only IIF was performed, in others only ELISA, and in some both IIF and ELISA. The largest group is that in which the ELISA with BPAg2 was performed. The titers of the anti-BMZ antibodies are presented in the total number of patients studied, levels prior to treatment and at the end of the study period. Statistical analysis was not possible in comparing the antibody levels in the various groups because of differences in the assay techniques and the methodologies used in different studies. However, it is clear that after treatment in the majority of patients there is a reduction in the antibody titer by IIF and BPAg2 ELISA, and by IB testing. Different authors have used different criteria for determining the positive values for the ELISA for BPAg2, based on the technique and kit used. Therefore, the authors considered the tests positive or negative as described in their individual reports.
Fig. 1. Comparison of serological data using indirect immunofluorescence (IIF) on monkey esophagus (ME) and human skin (HS) and enzyme-linked immunosorbent assay (ELISA) or immunoblotting (IB) of two different bullous pemphigoid antigen (BPAg1 or 2) prior to therapy and at the end of the study period. In some patients only IIF was carried out, in others only ELISA, and in some both IIF and ELISA. The titers of anti-basement membrane zone (anti-BMZ) antibodies are presented in the total number of patients studied, levels prior to treatment and at the end of the study period. In a sinificant majority of the patients there is a reduction in the antibody titer after treatment as detected by IIF, ELISA, and IB. Data compiled from refs 12, 16, 17, 19–24.
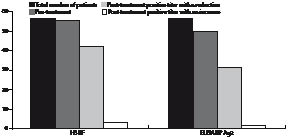
In 56 patients (39.1%) sera were evaluated using both IIF and ELISA BPAg2 (12, 20, 23, 24). The comparison of these data is presented in Fig. 2. In these patients the anti-BMZ antibody titers by IIF using NHS is compared with BPAg2 ELISA values. These data are compared in the total number of patients pre-treatment and at the end of the study period, indicating an increase or decrease in the antibody titer.
Fig. 2. Sera were evaluated in 56 patients using both indirect immunofluorescence (IIF) and enzyme-linked immunosorbent assay (ELISA) BPAg2. In these patients the anti-basement membrane zone (anti-BMZ) antibody titers by IIF using human skin (HS) are compared with BPAg2 ELISA values. These data are compared for the total number of patients pre-treatment and at the end of the study period (12, 20, 23, 24).
Using a Student’s t-test the difference between the values in the two tests in the three study groups were not statistically significant (p < 0.05).
Information on the initial treatment divided into treatment groups was available for only six studies (12, 16, 19, 20, 22, 23), which included 80 patients (55.9%). The numbers of patients in each category were as follows: 41 patients were treated with corticosteroids (51.25%) only, 27 patients with corticosteroids and immunosuppressive agents (33.75%), 12 patients with anti-inflammatory agents (15%), 7 patients with topical steroids only (8.75%). The results for the serological studies were recorded for each study simultaneously. In three studies (17, 21, 24) such information could not be obtained from the data provided. In one study all patients received corticosteroids and the number that received immunosuppressive drugs was not clear (24). In the second study data was available only on IB but not on IIF or ELISA (21). In the third there was a lack of description of subgroups of patients in whom serological studies were performed (17).
DISCUSSION
This analytical review presents data on 143 patients with BP who fulfilled the inclusion criteria. These patients were treated with a large spectrum of systemic agents. All patients improved at the end of the study period, though some were still on systemic therapy, while in others it was discontinued. The total length of therapy ranged from 2 to 144 months, but was not available for all patients.
Since an essential criteria for inclusion in the analysis was a positive DIF, this study provides the opportunity to address the likelihood of the presence of detectable levels of anti-BMZ antibodies only when the DIF is positive. While this is a limitation of this study, most dermatologists consider a positive DIF essential for the diagnosis of BP.
When IIF is performed prior to initiating systemic therapy, using ME and NHS (standard or salt-split), 82.2% and 98.2% of patients, respectively, are positive. ELISA for BPAg2 is positive in 91.5% of patients and the IB assay identified antibodies to BPAg2 in 90% of the patients tested and to BPAg1 in all the patients. Therefore, it appears that when DIF is positive there is statistically no significant difference in the likelihood of detecting anti-BMZ antibodies using IIF, ELISA or IB.
Until 2004, discussion on the comparison of the sensitivity between ELISA and IIF for measuring antibodies in BP sera was confusing because different technologies were employed (25, 26). Since 2004 a commercial ELISA to measure antibodies to BP180=BPAg2 (NC16a domain) has been available, and several authors have utilized this standardized assay and described its sensitivity (23, 27, 28). While no International Consensus Development conference has been organized to debate and define this issue, reading the literature there appears to be an informal agreement between authors that ELISA has greater sensitivity for antibodies in BP, compared with IIF (29, 30).
Analysis of the data highlight several important observations that have clinical relevance and consequence. At the end of the study period, (i) although there was a reduction in the titers sera studied by IIF using ME and NHS as substrate still had demonstrable levels of anti-BMZ antibodies in 29% and 75%, respectively. (ii) In three patients (7.1%) an increase was detected by human skin-immunofluorescence, of which one patient still had mild disease (20). (iii) Using the BPAg2 ELISA, 67.6% of patients tested had positive levels, though the levels were decreased; among these patients only eight had still mild disease at the end of the study period. In one patient (2.1%) an increase in the ELISA value was observed and this patient had mild disease at the end of the study period (20). These data collectively suggest that in the group of patients with BP studied, it appears that a serological remission does not accompany a clinical remission. In the small number of patients preliminary observations would suggest that amongst the assays used to determine the anti-BMZ antibody titers at the beginning of the therapy, and at the end of the study period, it would appear that the best correlation, if any, is observed in IIF with ME. Hence, there is a significant value in doing serological studies in BP patients prior to therapy. The value and benefits of such study during the clinical course or at the time of clinical remission might require further studies and follow-up. The authors of the present paper realized that the substrates used in the IIF might influence results. This is particularly true for ME and NHS. However, the ELISA is based on the NC16a extracellular domain of BP180, and several authors have demonstrated its value in the BP (19, 22, 31, 32). Other investigators suggest that additional epitopes in the intracellular and extracellular portion of BP180 might be useful if included in the ELISA (33, 34). Interestingly, in a small number of patients who developed recurrence of the disease, a rise in the levels of BPAg2 detected in the ELISA were observed, demonstrating that this might be of some predictive value in clinical management (12, 16, 19, 20, 24).
The presence of anti-BMZ antibodies in the absence of clinical disease opens an avenue for research into the role of these antibodies in the pathogenesis of the disease. While there is minimal data to provide any explanation, three possibilities exist. The first is the phenomenon of “epitope spreading” (34). Secondly, the subclass of the IgG and a switch between the subclasses may play a role (35–37). Thirdly, long-lived plasma cells may produce non-pathogenic antibodies (38). Such cells have immunological memory and may be sequestered in the bone marrow or spleen (39), where they may survive for long periods. Such cells are frequently resistant to conventional immunosuppressive therapy (40, 41) and rituximab (42).
An additional four different studies have demonstrated that serum levels of anti-BPAg2 antibodies detected by ELISA appear to parallel the disease activity (43–46). This trend was demonstrated in all IgG subclasses (45). However, these studies were not included in our analysis because they did not fulfill the inclusion criteria.
The levels of presumed pathogenic autoantibody do not necessarily reduce or disappear in several autoantibody-mediated diseases. In some recent studies in certain disease, such as proteinase-3-associated vasculitis (47), Graves’ disease (48) and multiple sclerosis (49), there appears to be a good correlation between clinical remission and marked reduction or absence of detection of pathogenic autoantibody. However, in other diseases, such rheumatoid arthritis and systemic lupus erythematosus, such distinct correlations are not always present (50, 51).
The effect of therapy on antibodies was described clearly in only one study (12). In this study antibody titers decreased in patients on corticosteroids, while those on other anti-inflammatory drugs showed minimal or no change. This would indicate that initial and subsequent therapy could affect antibody status at the end of the therapy. This was the trend in some studies (16, 19), but not in others (20, 22, 23). Taken collectively, a definitive influence of initial and subsequent therapy on the IIF and ELISA results during clinical remission cannot be made. The data is scanty, incomplete and lacks sufficient detail. Nonetheless, it appears that there is a trend to suggest that the incidence of lower titer of antibodies was observed in patients treated with corticosteroids and/or immunosuppressive agents compared with these on other anti-inflammatory agents.
In the opinion of the authors the analysis of the data provides some relevant and important clinical insights into the management of BP. However, there are some limitations that need to be addressed. First, the procedures for IIF are not standardized or uniform. Secondly, information on pathology and immunopathology is limited. The third limitation is the lack of uniform data on disease severity. Fourthly, there is a lack of long-term follow-up in the majority of studies. Fifthly, there is a lack of standardized statistical analysis. Each author has chosen to use a different statistical method to analyze their data (17, 20). Performing statistical analysis on the 143 patients in this review would be inaccurate. Therefore we have refrained from statistical comparisons of the data in this paper.
In conclusion, the questions addressed by us can be answered as follows: (i) there is a high incidence of the presence of anti-BMZ antibodies in patients with BP prior to the initiation of therapy. When the patients are in apparent clinical remission 30–50% have the presence of detectable levels of anti-BMZ antibodies, although the titers are decreased. (ii) The data provided by the investigators individually and collectively do not permit meaningful analysis of the correlation between the disease severity and the levels of anti-BMZ antibodies. (iii) In a limited and preliminary manner, it appears that immunosuppressive therapy reduces the auto-antibody titers more effectively than does pure anti-inflammatory therapy alone.
ACKNOWLEDGEMENTS
The authors are grateful to Olga Lyczmanenko, BA, MA, MLIS, library manager and Christopher Vaillancourt, BA, MA, MLIS of the Woodard Library of the New England Baptist Hospital for their assistance in the preparation of this paper.
The authors declare no conflict of interest.
REFERENCES