Alessandro Di Stefani1, Massimo Gabellini2, Amedeo Ferlosio1, Luigi Giusto Spagnoli1, Sergio Chimenti2 and Augusto Orlandi1*
1Institute of Anatomic Pathology and 2Department of Dermatology, University of Rome Tor Vergata, V.le Oxford 81, IT-00133 Rome, Italy. *E-mail: orlandi@uniroma2.it
Accepted December 1, 2010.
Proteus syndrome is a rare and complex congenital hamartomatous disorder with multi-organ involvement, characterized by a protean clinical phenotype that can be misdiagnosed. We report here a case of Proteus syndrome, with emphasis on the clinico-pathological findings of cerebriform plantar hyperplasia, which is crucial for a correct diagnosis and consistent patient management.
CASE REPORT
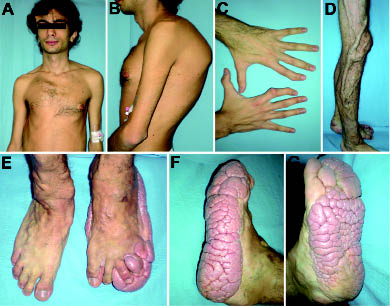
A 23-year-old man presented with severe discomfort and walking limitation caused by a slowly growing plantar mass, associated with various skin and bone abnormalities. The patient reported as earliest manifestations in the first months of his life the appearance of multiple reddish telangiectasias of the right leg and the lower lip. Over time the lip lesions regressed spontaneously, whereas those on the leg gradually enlarged, becoming prominent veins. At the age of 3 years, due to the increasingly evident disproportionate growth of the limbs and the macrocephaly with exostosis formation, an initial diagnosis of Proteus-like syndrome was suggested. In the following years there was a progressive manifestation and worsening of various skin and bone abnormalities, affecting the face, trunk and limbs, until the configuration of the actual complex phenotype. In addition, the patient reported a history of thrombosis of the left femoro-popliteal and saphena veins. The condition was sporadic in the family. Clinical examination revealed the presence of an asymmetric face, dysmorphic skull with frontal-parietal hyperostosis, hypertelorism, strabismus, long neck and low-set anteverted ears (Fig. 1A). His thorax was dysmorphic with dropped shoulders, anomalous orientated scapulae, scoliosis and stiff spine (Fig. 1B). Multiple abdominal lipomatous formations, diffuse axial and peripheral hypotonia and hypotropy were also evident (Fig. 1A, B). The hands were unequally developed, with the right hand smaller than the left, arachnodactyly and deformities of the second fingers (Fig. 1C). The limbs were characterized by disproportionate overgrowth, with the left leg shorter than the right, dermal hypoplasia, and ectatic veins (Fig. 1D). Moreover, his feet had a convolute thickening of the plantar surface, with a gyrate and cerebriform aspect, which was more prominent on the left side (Fig. 1E–G). This complex phenotype was consistent with the diagnosis of Proteus syndrome (1). In addition, echocardiography revealed tricuspid insufficiency, thoracic computed tomography imaging documented bullous emphysema, and abdominal magnetic resonance imaging gut angiolipomatosis. Patient cognitive functioning was unaffected. Since the cerebriform plantar hyperplasia of the left soles caused walking impairment, repeated trauma and infections, a selected surgical reduction was performed. The histopathological examination revealed extensive sclerosis of reticular dermis with broadened collagen bundles, sparse fibroblasts and no elastic fibres (Fig. 2A). Based on these findings, the diagnosis of plantar connective tissue naevus collagen type (or collagenoma) was established. Transmission electron microscopy confirmed the prevalence of thickened and irregular collagen bundles, packed in fibrils with homogeneous size, and marked reduction in elastic fibrils (Fig. 2B). Genetic investigation was not performed.
Fig. 1. Clinical presentation of Proteus syndrome. (A) Asymmetric face, frontal-parietal hyperostosis, long neck, low-set antiverted ears and diffuse hypotonia; (B) dropped shoulders and scoliosis; (C) aracnodactyly, with the right hand smaller than the left and deformities of the second fingers; (D) dermal hypoplasia and ectatic veins of the leg; (E–G) typical cerebriform plantar hyperplasia from different perspectives: note the diffuse and gyrate thickening of the plantar surface of the left feet.
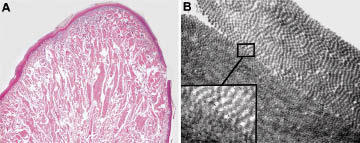
Fig. 2. Histopathological and ultrastructural findings of the cerebriform plantar hyperplasia. (A) Microscopic examination of haematoxylin and eosin (H&E) stained sections reveals hyper-orthokeratosis, flattening of the epidermis, and extensive sclerosis of reticular dermis with thickened and broadened collagen bundles. (B) Transmission electron microscopy shows collagen fibres densely packed in variably oriented bundles. Insert: a detail of homogeneously-sized collagen fibrils section. Original magnification: (A) ×20; (B) ×10,000.
DISCUSSION
Proteus syndrome is a rare, complex congenital hamartomatous disorder, originally described by Cohen & Hayden in 1979 (2) and named “Proteus syndrome” by Wiedemann and co-workers in 1983, after a minor Greek divinity who had the power to change his appearance at will (3). The diagnosis of Proteus syndrome is based on the presence of mandatory general criteria (mosaic distribution of lesions, progressive course, sporadic occurrence), in association with specific clinical findings with variable diagnostic importance (1, 4). Among these, the presence of connective tissue naevus, typically localized on the soles, also named “cerebriform plantar hyperplasia” is one of the most frequent (1, 4). Cerebriform plantar hyperplasia can be sporadic or acquired and, although not pathognomonic, is considered the sign with the greatest impact for the diagnosis of Proteus syndrome (4). It is not present in those disorders to be considered in the differential diagnosis, such as neurofibromatosis, Klippel-Trenaunay-Weber syndrome, Maffucci syndrome and Bannayan syndrome (4). Conversely, collagenomas are commonly encountered in other genetic disorders, such as Busche-Ollendorff syndrome, a rare autosomal-dominant condition, resulting from nonsense mutation in the LEMD3 gene (5) which encodes for a potent negative regulator of bone morphogenic protein and transforming growth factor-β signalling pathways (6). Recently, a mutation in LEMD3 has been reported also in familial cutaneous collagenomas (6). The genetic bases for the development of Proteus syndrome remain to be clarified. A post-zygotic mutation has been postulated (7). PTEN was considered a promising candidate gene because of its role in other hamartomatous syndromes (8). Germline PTEN mutations have been identified in some patients with overgrowth abnormalities with features of Proteus syndrome, but the diagnosis has since been disputed (9). It is likely that a PTEN heterozygous mutation alone is not enough to result in Proteus syndrome and a second “hit” in specific tissues or at a specific stage of embryological development and/or the involvement of several genes are needed (7). Thus, we hypothesize that loss of LEMD3 function mutations might be related also to the abnormal growth of connective and bone tissues, typical of Proteus syndrome. Moreover, the characteristic ultrastructural findings of our patient’s cerebriform plantar hyperplasia, with irregular bundles of collagen packed in fibrils with homogeneous size (Fig. 2B), differ from those reported previously (2) and can be consistent with phenotypic variation of the disease, due to different mutations and/or different involved genes.
REFERENCES