Christian Grønhøj Larsen and Jacob P. Thyssen*
Department of Dermato-Allergology, Copenhagen University Hospital Gentofte, University of Copenhagen, DK-2900 Hellerup, Denmark. *E-mail: jacpth01@geh.regionh.dk
Accepted April 12, 2011.



Christian Grønhøj Larsen and Jacob P. Thyssen*
Department of Dermato-Allergology, Copenhagen University Hospital Gentofte, University of Copenhagen, DK-2900 Hellerup, Denmark. *E-mail: jacpth01@geh.regionh.dk
Accepted April 12, 2011.
Penile pyoderma gangrenosum (PPG) is an uncommon, non-infectious and idiopathic skin disease. Therapeutic options include topical or systemic corticosteroids or other systemically administered immunomodulatory drugs (1). We described here an eruption of pustular PPG, which was treated successfully with topical tacrolimus.
CASE REPORT
A previously healthy 47-year-old Caucasian man was referred with an erythematous, vesiculo-pustular, sharply demarcated tumour, measuring 2×2 cm, located on the glans penis (Fig. 1A). The lesion developed over a 2-week period. The patient denied extramarital sex during the preceding year. Further physical examination was unremarkable. The tumour was unresponsive to topical Fucicort® therapy (betamethasone 1 mg/g and fucidin 20 mg/g) twice daily for nearly 2 weeks, followed by oral fluconazole treatment 50 mg daily in combination with topical mupirocin 2% ointment twice daily for a period of 2 weeks; a regimen that was commenced because bacterial and fungal infection could not be ruled out. A 3-mm punch biopsy was obtained aseptically from the lesion. It was culture-negative for bacteria, mycobacteria and fungus. Full blood screening revealed normal complete blood counts, renal and liver enzymes, rheumatoid factor, antinuclear antibodies, antiphospholipid antibodies (Wasserman’s reaction) and Borrelia antibodies. An elevationwas found of p-triglyceride: 18.3 mmol/l (≤ 2.0), p-cholesterol: 8.0 mmol/l (≤ 5.0), HbA1c fraction: 0.10 % (0.04–0.06) and p-glucose: 14.6 mmol/l (< 7.0). Based on the clinical picture and the histological examination of two 3-mm punch biopsies obtained with 1-week interval revealing epithelial hyperplasia and acute inflammation (Fig. 2), the patient was suspected of having pustular PPG in combination with undiagnosed diabetes mellitus (T2DM) and severe hyperlipidaemia. Therapy with topical tacrolimus 0.1% ointment twice per day was prescribed and resulted in a rapid and significant removal of the tumour after only 7 days of treatment (Fig. 1B) and almost complete elimination after 28 days (Fig. 1C).
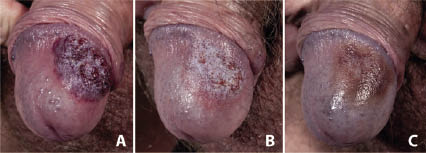
Fig. 1. Penile pyoderma gangrenosum. (A) Before treatment. (B) Improvement after one week of topical tacrolimus treatment twice per day. (C) Improvement after 4 weeks of treatment.
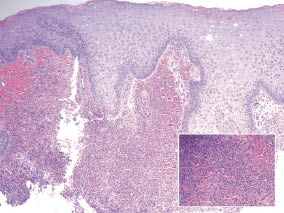
Fig. 2. Glans biopsy (and enlargement of the biopsy; inset) from the glans penis in a patient suspected of penile pyoderma gangrenosum shows epithelial hyperplasia and acute inflammation. Hematoxylin and eosin × 10, insert × 40.
DISCUSSION
A diagnosis of pyoderma gangrenosum is challenging and relies on clinical features as no specific serological or histopathological test is available (2). In approximately 50% of patients, the disorder is associated with underlying disease, e.g. rheumatoid arthritis, inflammatory bowel disease, haematological and lymphoreticular malignancies or immunosuppressive conditions (3). Four clinical variants of pyoderma gangrenosum have been described: ulcerative, bullous, vegetative, and pustular. The last is a relatively uncommon variant showing vesiculo-pustular lesions that do not ulcerate. The condition is most commonly observed in patients with active colitis ulcerosa and is located on the extremities and upper trunk (4). In 2 of 15 previous reports of PPG, an underlying disease was reported (5). Pustular PPG in combination with hitherto undiagnosed hyperglycaemia and hyperlipidaemia has so far not been reported. A patient with ulcerative PPG, who at the same time had well-treated T2DM and hyperlipidaemia, was found to be responsive to treatment with an 8-week course of prednisone (6). In addition, short-term therapy with topical tacrolimus was effective in a patient with the ulcerative variant (7).
One week of topical tacrolimus therapy was effective in a patient with pustular PPG and this treatment is recommended as a first-line modality for these patients. Surgical debridement is not recommended in the acute stage due to risk of tissue progression (8). The case described here emphasizes that screening for concomitant systemic diseases should be a prerequisite in patients with PPG.
ACKNOWLEDGEMENT
Henrik Klem-Thomsen is acknowledged for histopathology services.
The authors declare no conflicts of interest.
REFERENCES

