Tadashi Karashima, Keiko Hashikawa, Fumitake Ono, Hironobu Eguchi, Takahiro Hamada, Norito Ishii, Teruki Dainichi, Shinichiro Yasumoto, Daisuke Tsuruta and Takashi Hashimoto*
Department of Dermatology, Kurume University School of Medicine, and Kurume University Institute of Cutaneous Cell Biology, 67 Asahimachi, Kurume, Fukuoka 830-0011, Japan. *E-mail: hashimot@med.kurume-u.ac.jp
Accepted October 19, 2011.
Since Bowen’s disease, an intraepidermal squamous cell carcinoma, occurs frequently in elderly people, surgical treatment is sometimes difficult. Therefore, an alternative treatment is required due to other underlying diseases. We report here the case of an elderly man with Bowen’s disease who declined surgical treatment due to concerns of postoperative bleeding secondary to anticoagulation. Occlusive dressing therapy with maxacalcitol, an active vitamin D3 derivative, resulted in clinical resolution. We investigated the mechanism of anti-tumour activity of this vitamin D3 ointment in Bowen’s disease.
CASE REPORT
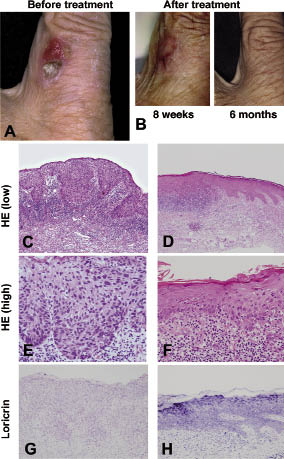
An 82-year-old man visited our hospital, with an asymptomatic erythematous tumour in the left index finger. He was on oral warfarin due to coronary artery disease, and had spinal canal narrowing, an abdominal aneurysm, and chronic renal failure. Over one year, the skin lesion had gradually enlarged and protruded. On examination, a cutaneous horn-like nodule adjacent to an erosion on slightly palpable well-circumscribed hyperkeratotic erythema was seen on the left index finger (Fig. 1A). There was no regional lymphadenopathy.
A 3-mm punch biopsy without cauterization was taken from the centre of the lesion. Histopathology revealed irregularly thickened epidermis composed of tumour cells with basophilic cytoplasm (Fig. 1C, E). Intercellular bridges were unclear, and basophilic nuclei and disarray in polarity were seen in the tumour cells. Multinuclear cells were also sporadically observed. There were no clefts in the basement membrane zone. Inflammatory cell infiltration of lymphocytes was observed in the upper dermis. Based on the above findings, the diagnosis of Bowen's disease was made. There was no spontaneous regression after the punch biopsy.
The patient did not wish to undergo surgical treatment or cryotherapy and had a number of complications that led to the decision not to perform surgery. As topical imiquimod and photodynamic therapy were unavailable in Japan at the time of his appearance, and as 5-fluorouracil has a side-effect of bone marrow suppression, we attempted topical application of maxacalcitol using Saran Wrap® once a day with the patient’s approval. The clinical course of the lesion was photographed (Fig. 1B, left). The cutaneous horn-like nodule first began to exfoliate, and the skin lesion gradually decreased in size. Six weeks after the initiation of the treatment, only a small patch of erythema remained. In contrast to the initial biopsy, a biopsy taken from the centre of erythematous lesion demonstrated a regressed tumour mass comprising regularly oriented cells with eosinophilic cytoplasm and slightly larger nuclei (Fig. 1D, F). We observed epidermal structure regenerating from both sides, which appeared to encompass the tumour tissue section. Lymphocytic infiltration was still observed in the upper dermis. Expression of loricrin was recovered (Fig. 1H). We completed the treatment in 8 weeks. During the course, there were no abnormalities in laboratory tests, including serum calcium level (8.74 mg/dl before the treatment, 8.84 mg/dl after the treatment; normal 8.7–10.3 mg/dl). No recurrence of tumour was observed 6 months after the initial treatment (Fig. 1B, right).
Fig. 1. (A) Skin lesion on the left index finger. (B) Consecutive clinical pictures after maxacalcitol occlusive dressing therapy. (C-F) Histopathological features of the primary lesion (C, E) and the lesion 6 weeks after the treatment (D, F) (Haematoxylin-eosin staining, (C, D): ×100, (E, F): ×400. (G, H) Immunohistochemical staining of loricrin in the primary lesion (G), and in the lesion 6 weeks after the treatment (H) (×100).
As digital Bowen's disease is known to be associated with human papilloma virus (HPV) infection (1, 2), we investigated the presence of HPV DNA. PCR for DNA extracted from a paraffin section, and in situ PCR were performed using degenerative primers to detect cutaneous type HPV (3, 4). PCR primers for β-globin were used as positive control (5). No cutaneous type HPV was detected by either analysis (data not shown).
Then, we investigated the presence of apoptotic cells in biopsy specimens using Derma™ TACS kit (Trevigen, MO, USA), as several synthetic vitamin D derivatives inhibit the growth of carcinoma cells by inducing apoptosis (6). Unexpectedly, apoptotic tumour cells were detected in the sections of the original lesion, but not in the lesion 6 weeks after the treatment (data not shown).
Finally, we performed immunohistochemistry for involucrin and loricrin as epidermal differentiation markers, and CD4, CD8 and CD20 as lymphocyte markers. Expression of involucrin in the tumour cells was weak both before and after application of maxacalcitol (data not shown). In contrast, pretreated tumour cells showed minimum loricrin expression. Loricrin was strongly expressed in the skin after maxacalcitol treatment (Fig. 1G). The expression of CD4, CD8 and CD20 in inflammatory cells infiltrated in the upper dermis was unchanged before and after the treatment (data not shown).
DISCUSSION
Vitamin D is the major regulator of calcium homeostasis (7). Most active vitamin D is an active form of vitamin D3, calcitriol (1α,25-dihydroxyvitamin D3) (7). Vitamin D enhances calcium and phosphate absorption from the intestines to maintain their correct blood concentrations (7). Vitamin D also has anti-proliferative, pro-differentiating, anti-inflammatory and immunomodulatory activities (7). In addition, anti-cancer actions of vitamin D have been studied in breast, prostate and colon cancers (7–9). In this study, we successfully treated a patient with HPV-unrelated Bowen's disease with maxacalcitol, a vitamin D3 analogue, which is a major drug in the treatment of psoriasis (10).
In order to elucidate the mechanisms of the anti-cancer effect of maxacalcitol in Bowen's disease, we performed DNA analyses of HPV, in situ detection of apoptotic cells and several immunohistochemical studies. The results revealed that Bowen’s disease in this patient was not caused by HPV infection. The regression of the tumour was not considered to be induced by apoptosis, because no apoptotic tumour cells were seen after maxacalcitol treatment. Rather, induction of differentiation may exert the therapeutic effect, because expression of loricrin was significantly enhanced after the treatment. However, immunomodulatory effects of maxacalcitol could not demonstrated by immunohistochemistry using anti-CD4, CD8 and CD20 antibodies.
ACKNOWLEDGEMENTS
We greatly appreciate the technical assistance of Ms Ayumi Suzuki, Ms Takako Ishikawa, and Ms Sachiko Sakaguchi, and the secretarial work of Ms Akiko Tanaka, Ms Yasuko Nakayama, Ms Emiko Hara, Ms Hanako Tomita, Ms Motoko Fukamachi, and Ms Mihoko Ikeda.
The authors declare no conflicts of interest.
REFERENCES