Lene F. Sandvik1,2, Petra Vogelsang1, Torbjørn Leivestad3, Roland Jonsson1 and Silke Appel1
1Broegelmann Research Laboratory, The Gade Institute, University of Bergen, NO-5021 Bergen, 2Department of Dermatology, Haukeland University Hospital, Bergen, and 3Institute of Immunology, Oslo University Hospital Rikshospitalet, Oslo, Norway. E-mail: lene.sandvik@gades.uib.no
Accepted November 30, 2011.
Organ transplant recipients are at high risk of developing squamous cell carcinoma (SCC) (1–3). These viral-associated skin cancers cause severe morbidity and may also be life-threatening (4, 5). Thus, regular follow-up by a dermatologist is recommended. The time intervals of the examinations should be determined by the individual’s risk for SCC development (6–8). One of the main risk factors is long-term immunosuppression (3, 9), leading to severe deficits in immunosurveillance.
Dendritic cells (DC) play an important role in immuno- surveillance, even though they constitute only 0.5% of the leukocytes in blood (10). Plasmacytoid DC (pDC) are a subset of DC. They produce interferon-alpha (IFN-α) and are considered to play a critical role in antiviral immunity (11). Type 1 myeloid DC (mDC1), another DC subset, are responsible for induction of T-cell responses (12).
On the basis of the potential of DC to prevent cancer development, we wanted to determine whether renal transplant recipients (RTR) who develop SCC have a reduced quantity of these two DC subgroups in blood compared with RTR who do not develop SCC.
MATERIALS AND METHODS
The Norwegian Renal Registry was utilized as source to RTRs living in Hordaland County in Western Norway. All adult RTR transplanted more than 8 years ago received a written invitation to participate in the study in January 2009 (112 subjects). Two enquiries did not reach the recipients. Sixty-one RTR (56%) gave their informed consent. The Norwegian Cancer Registry and the patients’ medical records were used to collect data on the occurrence of SCC and immunosuppressive medication. Fifteen out of 61 patients (25%) had excised one or more SCC. These 15 patients were matched to be as homogeneous as possible according to duration and type of immunosuppression (mean time after transplantation 22 years, range 9–36), age (mean age 63 years, range 51–74) and gender (male/female ratio 10:5), to 15 RTR without SCC (mean time after transplantation 20 years, range 9–33; mean age 65 years, range 52–79; male:female ratio 11:4).
One dermatologist performed a clinical examination of the 30 RTR to evaluate their skin type and presence of human papillomavirus-induced warts. All the participants had a good general condition, even though one patient without SCC was treated with antibiotics due to an infection. Subsequently, approximately 50 ml peripheral blood was collected in heparin tubes. The age- and gender-matched controls were 21 immunocompetent volunteers without SCC (mean age 64 years, range 50–78 years; male/female ratio 13:8).
The study was performed according to the Declaration of Helsinki, and was approved by the Regional Committee for Research Ethics (176.08) and the Data Inspectorate.
Staining of pDC and mDC1 was performed in heparinized blood stored at room temperature for less than 90 min. The DC were stained with the Blood DC enumeration kit (Miltenyi Biotec, Bergisch Gladbach, Germany), according to the manufacturer’s manual. Flow cytometry was performed on a BD FACSCanto I (BD Bioscience, San Jose, CA, USA) flow cytometer. Data analysis was performed with FlowJo software (Tree Star Inc., Ashland, USA). The results were calculated as percentage positive cells among leukocytes.
A 2-tailed Mann-Whitney test was used for the statistical analysis of pair-wise comparison between groups. The significance level was set at p < 0.05. The statistical analyses were performed using Prism (GraphPad Software Inc., La Jolla, CA, USA).
RESULTS
Patients with SCC had a reduced number of circulating pDC compared with patients with no SCC, without reaching statistical significance (0.057% vs. 0.079%). Moreover, the amount of pDC in both patient groups was significantly reduced compared with the controls (0.112%) (p = 0.0026 and p = 0.0077, respectively).
The amount of mDC1 in peripheral blood was similar in both patient groups and was reduced compared with the controls, albeit not statistically significant (patients with SCC = 0.060% and without SCC = 0.053% vs. controls 0.103%). The patient undergoing treatment for an infection had the highest mDC1-value (0.236% of leukocytes).
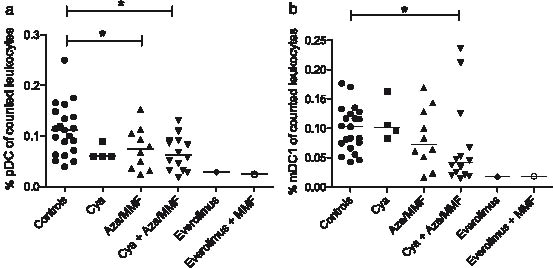
Since the patients were on different immunosuppressive medication, we analysed whether specific medication had an influence on the two DC subsets. The analysis revealed no such differences. Only 2 patients were treated with Everolimus, making statistical analyses impossible (Fig. 1).
DISCUSSION
To our knowledge, this study is the first to elucidate whether the quantity of pDC and mDC1 in peripheral blood of RTR might serve as a prognostic indicator for development of SCC.
We observed reduced amounts of pDC in the patients with SCC compared with the patients without SCC, although not statistically significant. An obvious reason for this could have been different medication in the two patient groups. However, comparing the patient groups according to which medication they were using revealed no statistically significant differences in the amount of pDC or mDC1 (Fig. 1). Also, the 2 patients treated with Everolimus did not deviate from the others, indicating that mTOR inhibition does not influence DC populations in a different way than conventional immunosuppression. Furthermore, it has been reported by Hackstein et al. (13) that it is mainly prednisolone in doses more than 10 mg/day that has a significant negative impact on pDC. In the present study the mean prednisolone dose was small in the patients with and without SCC (5.9 and 5.7 mg/day, respectively), making it unlikely that this caused the difference in pDC levels. Our study revealed a significantly reduced level of circulating pDC in the immunosuppressed patients compared with the immunocompetent control group, confirming the findings of Hackstein et al. (13).
Fig. 1. Differences in the type of medication do not significantly influence levels of dendritic cells (DC) in peripheral blood. Comparing different patient groups according to which medication they were using revealed no differences in the amount of plasmacytoid DC (a) and type 1 myeloid DC (b) between the patient groups. All the patients used prednisolone in addition (mean dose 5.76 mg/day, range 5–10 mg/day). The median is indicated by a line. Cya: cyclosporine A; Aza: azathioprin; MMF: mycophenolate mofetil. *p <0.05.
In our experiment there was no difference in the number of mDC1 in the 2 different patient groups and surprisingly no significant difference between the patients and the controls. This might be due to the limited number of patients included in this study. The high amount of mDC1 observed in the patient with an infection might reflect the increased antigen-presenting activity of the mDC1.
A reduced level of pDC would result in less secretion of IFN-α, thereby lowering the antiviral activity of the immune system. This might lead to reactivation of latent oncoviruses, finally resulting in increased incidence of viral-associated malignancies. Even though differences in pDC between the 2 patient groups did not reach statistical significant levels, we cannot rule out an association between development of SCC and a reduced amount of pDC in peripheral blood of immunosuppressed patients. A study encompassing a larger patient cohort is needed to support this data.
ACKNOWLEDGEMENTS
The authors would like to thank everybody participating in the study. We thank Dagny Ann Sandnes for excellent technical assistance, Einar Svarstad for distributing the enquiries to the patients and Arvid E. Nilsen for critical reading of the manuscript. This work was supported by the Bergen Research Foundation, Norwegian Cancer Society, and the Broegelmann Legacy. Some of the data in this article are from the Cancer Registry of Norway. The Cancer Registry of Norway is not responsible for the analysis or interpretation of the data presented.
The authors declare no conflicts of interest.
REFERENCES