Notalgia paraesthetica is a neuropathic pruritus on the back. The aim of this retrospective study was to examine patient characteristics in a consecutive cohort from Brazil and Germany. A total of 65 patients (49 women, 16 men; age range 25–80 years, mean 56.2 ± 12.7 years; median 57.0 years) were investigated in order to determine the spinal or peripheral origin of notalgia paraesthetica. Protein gene product 9.5-positive intraepidermal nerve fibers were significantly reduced in the pruritic compared with the non-lesional area (p < 0.05). In 32.3% of patients, radiological examinations showed a stenosis and in 47.7% a degeneration. A correlation between the radiological findings and the exact dermatomal localization of notalgia paraesthetica was found in 15.7% of the involved areas. The significant reduction in intraepidermal nerve fiber density suggests that damage to the peripheral nerves is a more important aetiological factor than spinal changes in notalgia paraesthetica. Key words: pruritus; itch; peripheral nerve; neuropathic pruritus; protein gene product 9.5.
(Accepted December 22, 2011.)
Acta Derm Venereol 2012; 92: XX–XX.
Sonja Ständer, Competence Center Chronic Pruritus, Department of Dermatology, University Hospital Münster, Von-Esmarch-Strasse 58, DE-48149 Münster, Germany. E-mail: sonja.staender@ukmuenster.de
Notalgia paraesthetica (NP), first described by the Russian neurologist Astwazaturow (1), is a unilateral chronic neuropathic pruritus on the back, mostly between the shoulders, located between the second and the sixth thoracic nerves (1–13). Given that the sensation may be composed of pain, pruritus, tingling, or pricking in the same area, the term NP unites the Greek terms notos (back), algos (pain) and paresthesias (1, 13). The clinical manifestation of NP varies from non-visible skin lesions to a circumscribed hyperpigmented macule, as found in the majority of patients, or a hyperpigmented patch. These different clinical findings resulted in different published terms, such as puzzling posterior pigmented pruritic patches (14), peculiar spotty pigmentation (15), hereditary localized pruritus (2), and macular amyloidosis (16–20), all of them basically describing the same phenomenon.
The aetiology of NP is not yet clearly understood, but is mostly attributed to compression of spinal nerves by thoracic spine abnormalities (12). Vertebral pathologies comprising, for example, nucleus pulposus herniation, osteophytes and, more frequently, degenerative changes, have been described to correlate with dermatomal localization of NP (11, 12). According to another hypothesis, sensory neuropathy of the posterior branches of the peripheral nerves induced by musculoskeletal compression (3, 4, 6, 7, 9, 13) is the cause of NP. The posterior dorsal rami of the thoracic nerves run a right-angle course through the muscles, and it has been suggested that this makes them more vulnerable to trauma and entrapment (4, 9). Several other factors have been described, including association with multiple endocrine neoplasia (MEN) 2A (7) or an intake of saccharin (5). The aim of this 2-centre study was to examine and correlate multiple clinical, cutaneous neuroanatomical and radiological characteristics of NP in a consecutive cohort of patients.
Methods
In total a cohort of 65 patients with NP, including 42 from Germany and 23 from Brazil, was analysed retrospectively (Table I). In Germany the database of the Competence Center Chronic Pruritus of the University Hospital Münster was searched for patients with NP. The database includes all patients with chronic pruritus who consulted the centre since March 2009. In Brazil 23 patients of the Department of Dermatology of the Jundiai Medical School in Sao Paulo were identified in the local database. Before data collection and analysis patients were informed and an informed consent form was signed. For determination of intraepidermal nerve fibers (IENF) patients signed an additional informed consent form. The study was approved by the local ethics committee.
Table I. Notalgia paraesthetica (NP): work-up in 65 patients
|
Investigation
|
Total cohort
n (%)
|
Germany
n (%)
|
Brazil
n (%)
|
|
Dermatological investigation
|
65 (100)
|
42 (100)
|
23 (100)
|
|
NP localization (in quadrants)
|
63 (96.9)
|
41 (97.6)
|
22 (95.6)
|
|
Dermatomal chart
|
22 (33.8)
|
22 (52.4)
|
n.a.
|
|
Pruritus assessment: quality
|
40 (61.5)
|
40 (95.2)
|
n.a.
|
|
Skin biopsy: histology
|
34 (52.3)
|
34 (81.0)
|
n.a.
|
|
Skin biopsy: IENF
|
21 (32.3)
|
21 (50.0)
|
n.a.
|
|
Radiology:
MRT
Computed tomography
X-ray
|
51 (78.5)
25 (38.5)
1 (1.5)
25 (38.5)
|
28 (66.7)
25 (59.5)
1 (2.3)
2 (4.8)
|
23 (100)
0 (0.0)
0 (0.0)
23 (100)
|
IENF: intraepidermal nerve fibers; MRT: magnetic resonance tomography.
The analysed parameters included demographic data, history and localization of NP, dermatological investigation, pruritus characteristics and therapy. Localization of pruritus was determined by: (i) dividing the back into quadrants (division in upper and lower back at T7); and (ii) identifying the exact corresponding dermatome in 22 patients by drawing the affected area in a dermatomal chart. Data obtained from routine investigations, such as radiological (n = 51) and histological (n = 34) examinations, and examination of the density of IENF (n = 21) were included. For counting the IENF, biopsies of lesional and non-lesional skin were processed for immunostaining with protein gene product (PGP) 9.5 in the laboratory of the Department of Dermatology of the University Hospital Münster, as described previously by Schuhknecht et al. (21). In brief, samples were fixed in 4% paraformaldehyde, thereafter in sucrose, and stored in liquid nitrogen. Cryosections were stained with a polyclonal antibody against the neurone-specific hydrolase PGP 9.5, anti-PGP 9.5 (rabbit 1: 2000; Chemicon, Temecula, CA, USA).
Statistical analysis
The data of the total collective was statistically analysed with Predictive Analysis SoftWare (PASW) (SPSS Inc., Chicago; 2009). The analysis was applied to all patients from whom data was available. Before statistical testing each continuous variable was analysed for its normal distribution using the Kolmogorov-Smirnov test. The significance of the difference between the lesional and non-lesional IENF values was tested with the Wilcoxon test. The relationship between the IENF values and the duration of pruritus was investigated with the Pearson correlation coefficient. To investigate the correlation between the duration of pruritus and hyperpigmentation (clinical and histological) and the duration and presence of scratch lesions and presence of amyloid, respectively, the Mann-Whitney U test was performed. The correlation between the IENF and the presence of scratch lesions and hyperpigmentation was also tested by the Mann-Whitney U test. The McNemar test was used to determine the correlation between the dermatome, affected by pruritus, and the lesion on magnetic resonance imaging (MRI). A 2-sided significance test was performed for all statistical tests and a p ≤ 0.05 was considered statistically significant.
Results
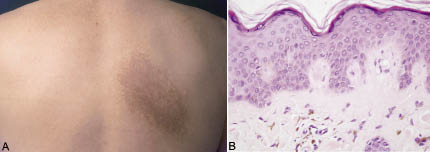
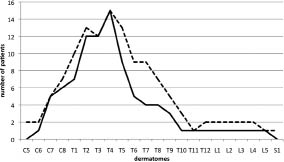
A total of 65 patients (49 women, 16 men; age range 25–80 years, mean 56.2 ± 12.7 years; median 57.0 years) with NP were evaluated (Table SI; available from http: //www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1344). The age of onset in 73.8% of patients was above 40 years (mean 49.5 ± 14.4 years; median 50.0 years) except in one patient who had early onset of NP at the age of 2 years, which was associated with MEN 2. Skin findings were distinguished by the presence of hyperpigmentation and/or scratch lesions (Table SI; Fig. 1A). Only 4 patients (6.2%) showed no skin lesions: neither hyperpigmentation nor scratch lesions (Fig. 1A). Statistical analysis with the Mann-Whitney U test revealed no correlation between the duration of pruritus and the presence of hyperpigmentation or scratch lesions (p > 0.05). The upper left and right quadrants were equally affected and were more often affected than the lower quadrants. The most frequently affected dermatomes were the dermatomes T2 (upper back, 13 patients, 20.0%), T4 (upper back, 15 patients, 23.1%) and T5 (upper back, 13 patients, 20.0%). Half (50.4%) of the cases showed that the pruritic dermatomes were found between T1 and T5. In the course of NP, the increase in numbers of affected dermatomes was 37.4% compared with the localization of NP in the beginning (Fig. 2).
Histological investigation
In 26 patients (40.0%) epidermal hyperpigmentation and in 28 patients (43.0%) dermal hyperpigmentation of basal keratinocytes and melanophages in the papillary dermis were prominent in the histological investigation. Amyloid deposits in the papillary dermis were found in 6.1% (Fig. 1B). In statistical analysis the Mann-Whitney U test showed no significant correlation between the duration of NP and the histological presence of hyperpigmentation and amyloid deposits (p > 0.05). Determination of the epidermal nerve fiber density revealed a significantly reduced density in the pruritic area (mean 7.15 ± 4.3 fibers/mm; median 6.95 fibers/mm) compared with the anatomically identical, non-pruritic area (mean 10.3 ± 5.7 fibers/mm; median 9.7 fibers/mm) (p = 0.035). The duration of NP did not correlate significantly with the reduction in the IENF (p > 0.05). Furthermore, the Mann-Whitney U test revealed no significant correlation between the presence of scratch lesions or hyperpigmentation and the reduction in the IENF (p > 0.05).
Fig. 1. (A) Notalgia paraesthetica (NP) in the upper right quadrant of a 53-year-old man. NP had been present for a period of 5 years. Clinically, hyperpigmentation was present. (B) Histological investigation revealed dermal amyloid deposits, epidermal hyperpigmented keratinocytes and dermal melanophages. H&E staining, × 400.
Fig. 2. Dermatomal localization of pruritus at the beginning (black line) and in the course of notalgia paraesthetica (NP) (dotted line) in 22 patients. During the course of the disease, NP began to spread to neighbouring areas.
Radiological investigation
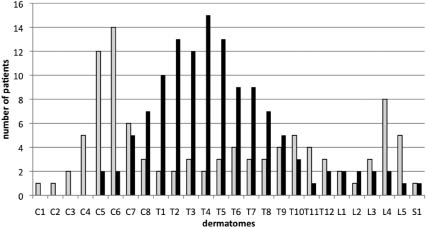
Radiological investigations showed stenosis of the spinal column and/or the neuroforamina in 21 patients (32.3%), degeneration in 31 patients (47.7%), and combinations of these in 14 patients (21.5%). Normal radiological findings were present in 13 patients (20.0%). The dermatomes C6 (14 patients, 21.5%), C5 (12 patients, 18.5%) and L4 (8 patients, 12.3%) were mainly affected (Fig. 3). In 19 patients from the German cohort who completed a dermatomal chart, the MRI findings could be correlated with the exact clinical dermatomal localization of the NP. In total 70 dermatomes were radiologically affected and 114 dermatomes clinically affected. In only 11 dermatomes (15.7%) the clinical presence of NP correlated with the radiologically detected localization of the lesion. Statistical analysis with the McNemar’s test revealed that only in 5 dermatomes (7.1%) was this correlation significant (p < 0.05). Thus, only in 5 dermatomes was pruritus associated with MRI detection of a lesion.
Fig. 3. Notalgia paraesthetica: distribution of dermatomal localization of pruritus (black) and radiological lesions (grey). The number of affected patients is presented for each dermatome.
Discussion
NP still represents an enigmatic disease with a lack of representative cohort studies. The aim of our study was the retrospective analysis of a consecutive collective against the background of current hypotheses about causes and contributing factors to NP. In addition, multiple clinical, histological and radiological parameters were statistically correlated in order to detect a connection between them. This study checked a total of 65 patients in a 2-centre collective of patients in Brazil and Germany with NP. With 51 patients who underwent a radiological examination and 21 patients with data for quantification of the intraepidermal nerve fiber (IENF) density, this study has examined the largest collectives concerning these 2 factors. The limitations of this study are the retrospective design, different radiological methods performed by different physicians, a missing control collective and the challenge to correlate objective radiological data with subjectively reported symptoms including the localization of NP. Given that NP is relatively rare (11), a controlled prospective study is still challenging to date.
In this study we have shown that there is no radiological proof for the presence of spinal abnormalities as the cause of NP, despite evidence for the neuropathic origin of NP. Degenerative, traumatic or compressing spine changes have been assumed to be aetiological for NP since 1997 (11–13, 22). For example, Savk et al. (11, 12) showed that, in up to 80% of patients, there were radiographic changes of the spinal cord; and in up to 60–70% of patients these correlated with the topographic localization of NP. Other authors (6, 10) described radiological lesions in NP patients without establishing a topographical correlation with NP. Degeneration (47.7%) or stenosis (32.3%) or a combination of both was shown by 58.5% of our patients. Degenerative and stenosing spine changes correlated topographically in only 15.7% of dermatomes to the exact dermatomal localization in NP. Moreover, statistical analysis revealed that the correlation was significant in only 7.1% of the affected dermatomes. In only 5 dermatomes the appearance of pruritus was found to be dependent on a lesion detected under MRI and was incidental in the other dermatomes. Our results suggest that the presence of spinal abnormalities do not necessarily explain the symptoms of NP and seems to be much less than assumed the cause of NP. These findings are in contrast with the results reported by Savk & Savk (12). This is even more remarkable, since they considered only the worst lesions detected by MRI and correlated this with the NP topographical area instead of single dermatomes. In accordance with this, we analysed our data according to the topographical NP area. Using this method, 9 of the 29 pruritic areas (31%) correlated with a lesion in the MRI. Recording the exact dermatomal localization of NP seemed to provide a possible explanation for the discrepancy. Moreover, degenerative changes of the spine were included in the topographical correlation in previous studies and also discussed in NP patients to be causal. These findings have not been compared with the radiological investigations of an age-matched control group (6, 10–12). Since neither they nor we included a control group, all studies should be interpreted with caution. Radiological studies showed that half of healthy volunteers have pathological radiological findings at the thoracic spine without any complaints (23). The degree of radiological changes was clearly age dependent (23). The presence of degenerative changes in NP may therefore be incidental until shown otherwise in a prospective study including an age-matched control group. Moreover, NP displays a circumscribed roundish pruritic area on the back, which does not follow the full length but only a small part of the innervated dermatome. In brachioradial pruritus, a neuropathic pruritus at the lower arm, the full length of the dermatome is symptomatic. Accordingly, 80% of all patients have a compression of neuronal structures at the cervical spine, explaining the localized pruritus on the arms (24). From the clinical point of view, the typical localization of NP does not seem to be correlated with a spinal cord compression. Since the radiological examination in our study was performed using different radiological methods and by different physicians, future prospective studies with a sensitive radiological examination and precise correlation with exact clinical localization of NP have to be carried out to prove or disapprove the speculation on the spinal involvement in the pathogeneses of NP.
Another hypothesis on the aetiology of NP focuses on altered dermal sensory innervation and sensory neuropathy of the posterior branches of the peripheral nerves (4, 6, 7, 9, 13, 25). Wang et al. (26) demonstrated thoracic nerve injury leading to serratus anterior dysfunction as the cause of NP in 4 patients. Electromyography showed evidence for paraspinal denervation suggesting nerve compression in another patient with NP (27). In addition, one patient developed NP after neuralgic amyotrophy; electromyography revealed no spontaneous activity in the muscles, while radiography of the spine was normal (28). These reports underline the hypothesis of a peripheral, but not a spinal, origin of NP. Injured peripheral nerves may fire spontaneously inducing pruritus or pain and show altered neuroanatomy in the skin (9). Of note, in our study, the number of dermatomes increased during the course of the disease, possibly reflecting involvement of neighbouring innervation territories of cutaneous nerves.
Previous immunohistochemical investigations showed an increased innervation in NP in individual patients (6, 29). For example, Springall et al. (6) reported in 5 patients a semiquantitative increase in PGP 9.5-positive dermal and epidermal nerve fibers, whereas neuropeptides such as substance P appeared normal. Fantini et al. (8) investigated the density of PGP 9.5-positive epidermal and dermal nerve fibers semiquantitatively. They found no differences in the presence, distribution and number of nerves in lesional compared with non-lesional NP skin in 8 patients despite a slight quantitative difference being inconsistently present. Given that sensory, unmyelinated epidermal nerve fibers have been described to be of major importance in pruritus induction (30, 31), we investigated for the first time the exact number of IENF by means of a highly sensitive method (21). According to our counting rules, only nerve fibers crossing the basement membrane are counted, whereas secondary intraepidermal branching is excluded from quantification. This assures valid data independently of the epidermal thickness, which may vary according to the patients´ scratching behaviour (32). We found a significantly decreased number of PGP 9.5-positive IENF in the lesional area compared with the non-pruritic, non-lesional area (p < 0.05). These findings are not in agreement with the previous immunohistochemical investigations (6, 8, 33). This discrepancy can be explained by the semiquantitative method used by others, without exact determination of the nerve fiber density using the focus floating microscopy. In our study, the decreased IENF did not correlate with different clinical parameters. These include the duration of the pruritus and the clinical presence of NP, which consisted of normal skin, hyperpigmentation or scratch lesions. The neuroanatomical change of IENF may therefore be related to the sensory neuropathy and, in addition, may itself contribute to the induction and maintenance of the pruritus in NP. For example, a decrease in IENF in prurigo nodularis (21) and uraemic pruritus (34) is discussed to be part of the pruritus. Accordingly, Schmelz et al. (35) could demonstrate spontaneous firing of damaged neurones in patients with chronic pruritus.
Finally, NP may be rarely linked to the autosomal dominant syndrome MEN type 2 A (7, 36, 37) and has therefore been attributed to heredity (“hereditary localized pruritus”; 2,7). In our collective, only one patient had familial MEN 2A with presence of NP. Interestingly, this patient developed NP as early as the age of 2 years, while the majority of our collective developed NP after reaching the age of 40 years. Our MEN 2A-positive patient demonstrated clinical hyperpigmentation with reduced intraepidermal nerve fiber density. Until now, it is unclear whether other patients with MEN 2A and associated NP also show reduced intraepidermal nerves. Interestingly, several cases report the association of macular amyloidosis with MEN 2A (38, 39), which was not a histological criterion in our patient. Development of a macular amyloidosis (“friction amyloidosis”) occurs as a result of scratching and filamentous degeneration of epidermal keratinocytes (20, 40–45). In macular amyloidosis, amyloid deposits were found histologically in the papillary dermis (18–20, 33, 36, 46, 47). Keratin filaments were present as eosinophilic amorphous masses in the papillary dermis without having any link to primary amyloidosis or deposits of immunoglobulins (20). In our collective, only 6.1% of patients exhibited amyloid deposits upon histological investigation. Clinically, these patients showed hyperpigmentation and they did not differ from those having no amyloid deposits but showing also hyperpigmentation. This is in line with previous reports (10, 18, 36), which found amyloid deposits in only a few patients. Others (6, 7,11, 33, 47–51) found no amyloid deposits in their patients. No correlation pertaining to the presence or absence of amyloid with any clinical parameter such as the duration or the localization of NP was revealed through our statistical analysis. It may be speculated that amyloid deposits in NP may depend on an aetiology-independent factor, such as scratching after keratinocyte damage, and being present only in some, but not all, areas of NP. Amyloid deposits may be just an incidental finding possibly depending on the area of skin biopsy. Proof of this hypothesis would require investigation of representative skin biopsies and serial sections. However, the previous assumption that the NP may be present in 3 clinic-histopathological states, namely: (i) normal skin, (ii) posterior pigmented pruritic patch, and (iii) macular amyloidosis (17, 18), is supported by our findings. Furthermore, the 3 states do not develop sequentially, but can occur independently of each other. This suggests that NP does not specifically require the presence of any one of these states. In addition to amyloid deposit, which is rather rare, histological examination revealed the presence of epidermal single-cell necrosis (36.9% of patients), dermal hyperpigmentation (43%) and a lymphocytic perivascular inflammatory infiltrate (47.7%), thus confirming previous reports (6, 8–11, 14, 18, 19, 22, 33, 36, 47–51).
If the working hypothesis is that the aetiology of NP is to be found in disordered peripheral nerves, it would make sense to assume that therapies targeting this factor will prove beneficial. Current therapeutic approaches comprise, for example, topical capsaicin including a novel 8% capsaicin patch (49, 52–55), anticonvulsants (6, 56, 57), injection of botulinum toxin (58), paravertebral local anaesthetic block (9), physical therapy (10), transcutaneous electrical stimulation (TENS) (59), peripheral nerve field stimulation (PNFS) (60), surgical decompression of the nerves (61), osteopathic manipulative treatment (62) and electrical muscle stimulation (EMS) (26). Although analysis of the treatment of NP was not the main aim of this study, it is of interest to note that, in agreement with previous reports, in our patients (data not shown) application of anticonvulsants appeared to be the most promising approach (6, 56, 57).
ACKNOWLEDGEMENTS
We thank Katharina Lotts and Rajam Csordas-Iyer for assistance in the preparation of the manuscript and Andrea Wissel for excellent technical assistance.
References