Takanori Hidaka, Taku Fujimura*, Akiko Watabe, Akira Hashimoto, Tahahiro Haga, Kaoru Onami, Masato Mizuashi and Setsuya Aiba
Department of Dermatology, Tohoku University, Graduate School of Medicine, Seiryo-machi 1-1, Aobaku, Sendai, 980-8574, Japan. *E-mail: tfujimura1@mac.com
Accepted January 12, 2012.
Primary cutaneous apocrine carcinoma (AC) is a rare and highly aggressive cutaneous adenocarcinoma. In general, most cutaneous AC occurs in the axilla and it is more common in middle-age women (1). Complete remission by chemotherapy is uncommon and median survival was only 2 years for patients with Bloom-Richardson grade 3 tumours (2).
HER-2 is a 1260-amino-acid transmembrane protein with tyrosine kinase that plays a central role in cell differentiation, adhesion and motility (3). In the treatment of breast cancer, HER-2 signal inhibitors, such as the humanized monoclonal antibody trastuzumab and the small molecule tyrosine kinase inhibitor lapatinib, have been used as a standard therapy for HER-2 overexpressing metastatic tumour (4). Moreover, several reports have indicated that the apocrine subtype of breast cancer consistently overexpressed HER-2 (5). Interestingly, AC has a marked histological similarity to the apocrine subtype of breast cancer, including immunohistochemistry (6). Therefore, we hypothesized that a HER-2 signal inhibitor, such as lapatinib, can be effective for HER-2 overexpressing metastatic AC.
We report here a patient with a metastatic AC showing a complete remission following the administration of lapatinib with capecitabine. To our knowledge, this is the first case report describing the successful treatment of metastatic AC with HER-2 signal inhibitors.
CASE REPORT
A 62-year-old Japanese man visited our outpatient clinic with a 3-year history of a bleeding nodule on his scalp. Physical examination revealed a dome-shaped, 45 × 40 mm, ulcerated nodule on the left side of his scalp (Fig. 1) and bilateral cervical lymph node swelling. Biopsy revealed that tumour cells proliferated mainly in the dermis, forming solid pattern nests and pagetoid epidermal upward migration, especially at the hair follicle (Fig. 2a). The tumour consisted mainly of neoplastic cells with abundant eosinophilic cytoplasm, large nuclei containing prominent macronucleoli and cytological pleomorphism (Fig. 2b). Immunohistochemically, these tumour cells were positive for cytokeratin (CK) 7, CK8, CK18, CK19, gross cystic disease fluid protein (GCDFP)-15, a1-AT, androgen receptors and HER-2 (immunohistochemistry (IHC) score of 3+), and negative for CK10, CK14, CK20, p63, CEA, CA19-9, HER-par-1, a FP and oestrogen receptor. Moreover, the cytoplasm contained periodic acid-Schiff diastase resistant granules. From these data, we diagnosed his tumour as an AC. Computed tomography (CT) scan from neck to abdomen revealed significant enlargement of cervical lymph nodes. There was no sign of distant metastasis. A cranial magnetic resonance scan did not show any sign of intracranial involvement. There was no evidence of an internal malignancy on screening CT scan.
Fig. 1. A dome-shaped, 45 × 40 mm, easy-bleeding nodule on the left side of the scalp.
Fig. 2. (a) Tumour cells proliferate mainly in the dermis, forming solid pattern nests and pagetoid epidermal upward migration, especially at hair follicle (H&E). (b) The tumour consists mainly of neoplastic cells with abundant eosinophilic cytoplasm, large nuclei containing prominent macronucleoli and cytological pleomorphism (H&E). Immunohistochemical staining for the primary tumour reveals that this tumour was positive for (c) gross cystic disease fluid protein 15 and (d) HER-2. a, c, d: × 100, b: × 400.
The tumour was excised with a 3-cm margin. Additional radiotherapy after surgical treatment was performed on left parietal and cervical regions, with a total dose of 70 Gy. One month after the surgical treatment, cisplatin (80 mg/m2 every 4 weeks) was administered combined with 5-fluorouracil (800 mg/m2 for 5 days for 2 cycles).
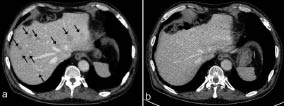
Five months after the tumour excision, the CT scan disclosed multiple liver nodules, which were suspicious of AC metastasis. Since the metastatic lesions appeared during the course of the chemotherapy, we considered that these metastatic lesions were resistant to both cisplatin or 5-fluorouracil. Therefore, considering that the tumour cells express HER-2 strongly, with an IHC score of 3+, we administrated trastuzumab, 2 mg/m2 every week. Three months after the administration of trastuzumab, the CT scan showed complete regression of all metastatic tumours. Nevertheless, liver metastasis reappeared 7 months after the administration of trastuzumab (Fig. 3a). We considered that his tumour had become resistant to trastuzumab. Therefore, we next administrated lapatinib, 1,250 mg once daily, combined with capecitabine 1,000 mg/m2 twice daily for 14 of every 28 days. No side-effects were observed, except for slightly general fatigue. Four months after the administration of this combination therapy, all the metastatic tumours disappeared, as observed on the CT scan (Fig. 3b). Six months after the remission of liver metastasis, his AC was still under remission.
Fig. 3. Computed tomography scan disclosed multiple liver metastasis of apocrine carcinoma (arrows) (a) before the administration of HER-2 signal inhibitors, and (b) 4 months after the administration of lapatinib combined with capecitabine.
DISCUSSION
Apocrine neoplasms are well-known carcinomas in the mammary glands (7) and it is difficult to distinguish breast cancer morphologically from cutaneous AC (6). Several reports suggest that HER-2 signal inhibitors can improve response rates, time to progression, and even survival in only HER-2 overexpressing type breast cancer, so the evaluation of Her-2/neu expression is indispensable for the use of HER-2 signal inhibitors (8–11). Indeed, Slamon et al. (12, 13) mentioned that approximately 25–30% of breast cancers overexpress HER-2, and HER-2 signal inhibitors are administered in the treatment of breast cancer as standard (4). Moreover, HER-2 overexpression is known to associate with an aggressive clinical course and a poor outcome in cases of apocrine subtype of breast cancer (12–14). Previously, Wick et al. (15) reported that approximately 30% of cutaneous ductal sweat gland carcinomas overexpress HER-2. In the present case, trastuzumab was administered to HER-2-positive metastatic AC and achieved complete, but temporal, remission. Furthermore, we achieved complete resolution of recurrent hepatic lesions with lapatinib and capecitabine treatment. This case indicates that HER-2 signal inhibitors are quite effective for HER-2-positive AC.
The authors declare no conflict of interest
REFERENCES