Takanori Hidaka, Taku Fujimura*, Akira Hashimoto and Setsuya Aiba
Department of Dermatology, Tohoku University, Graduate School of Medicine, Seiryo-machi 1-1, Aobaku, Sendai, 980-8574, Japan. *E-mail: tfujimura1@mac.com
Accepted January 21, 2012.



Takanori Hidaka, Taku Fujimura*, Akira Hashimoto and Setsuya Aiba
Department of Dermatology, Tohoku University, Graduate School of Medicine, Seiryo-machi 1-1, Aobaku, Sendai, 980-8574, Japan. *E-mail: tfujimura1@mac.com
Accepted January 21, 2012.
Dermatofibrosarcoma protuberans (DFSP) is a fibrohistiocytic tumour of intermediate malignancy characterized by slow infiltrative growth and a high tendency to recur locally. Pigmented DFSP, also known as Bednar tumour, is a rare variant of DFSP and accounts for up to 5% of all DFSPs.
DFSP occurs predominantly on the trunk, back and proximal extremities, with 12–15% of the cases localized in the head and neck region (1). When the lesions are located near critical facial structures, standard surgical therapy with a wide margin is impractical for cosmetic and functional reasons. We describe here the successful treatment of a pigmented DFSP on the nasal root with CyberKnife radiosurgery.
Case Report
A 37-year-old Japanese woman visited our outpatient clinic with a 2-year history of a subcutaneous nodule and severe tenderness in the nasal root. Physical examination revealed a skin-coloured, elastic, hard, subcutaneous nodule 10 × 10 mm in size that was fixed to the underlying tissues, and venous stasis at the bilateral sides of her nasal root (Fig. 1). No lymphadenopathy was detected in the cervical lymph nodes. The incisional biopsy specimen above the periosteum revealed the monomorphous proliferation of bland spindle cells with a storiform pattern, low mitotic activity and irregular infiltration into surrounding muscular and adipose tissues and deep margin involvement (Fig. 2a). There were many pigment-laden cells irregularly scattered among the tumour cells (Fig. 2b). Immunohistochemically, the spindle cells were positive for vimentin and CD34 and negative for factor XIIIa, HMB-45 and S-100 (data not shown). The COL1A1-PDGFB fusion gene was not detected by fluorescence in situ hybridization analysis. Magnetic resonance imaging revealed that the subcutaneous mass adjoined the underlying bone. From the above data, we diagnosed this patient as having pigmented DFSP without COL1A1-PDGFB fusion gene.
Fig. 1. A skin-coloured, elastic, hard, subcutaneous nodule 10 × 10 mm in size and venous stasis at the bilateral sides of the nasal root. The extent of induration is circumscribed with a dotted line.

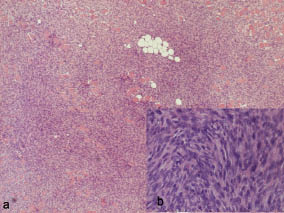
Fig. 2. (a) Subcutaneous tumour mass with irregular infiltration into the surrounding muscle and adipose tissues. (b) Monomorphous proliferation of bland spindle cells with a storiform pattern and pigment-laden cells irregularly scattered among the tumour cells. (Haematoxylin and eosin stained sections.) Original magnification a: × 100 and b: × 400.
As the lesion was adjacent to the eyes, we employed a CyberKnife (Accurray, Tokyo) for the initial therapy. The lesion was irradiated to as far as 2 cm from the margin of the tumour with 36 Gy in total, divided into 4 doses. One month after irradiation, the MRI showed complete remission of the tumour. Subsequently, MRI was performed every 2 months. Nine months after the complete remission, her DFSP was still under remission, and only mild dacryocystitis was observed as a side-effect.
Discussion
DFSP characteristically grows seemingly at random, with microscopic finger-like projections emanating from the centre of the tumour, sometimes for long distances (2). Due to their infiltrative natures, all DFSP variants have a high recurrence rate after standard surgical excision, ranging from 3.7% to 21% (3–5). Though Mohs micrographic surgery (MMS) for DFSP has an excellent recurrence rate of 1.5% (6), its labour-intensiveness limits the operable facilities. For above reason, the standard initial treatment for DFSP has been wide local excision at many facilities, and previously, Lindner et al. (6) advocated that a surgical margin of 2.5–3 cm was adequate to achieve local control.
When the lesion is located near critical facial structures, a wide surgical margin is not practical. As an alternative to wide resection, Lemm et al. (7) reviewed the literature about DFSP and suggested MMS, radiotherapy and molecular targeted therapy with imatinib as a therapy that could achieve complete remission. In our case, MMS was not feasible in our institution and imatinib would not be effective due to the absence of COL1A1 and PDGFB fusion genes, which leads to a constitutive activation of the platelet-derived growth factor receptor (8), which is inhibited by imatinib. In addition, although we reported previously that glucocorticoids suppress the growth of DFSP (9), glucocorticoids lack tumour-specificity and are unable to achieve complete remission.
For the above reasons, we selected CyberKnife for robotic image-guided stereotactic radiosurgery as the initial therapy. DFSP is regarded as a radio-responsive tumour, and indeed, several reports have suggested the successful treatment of DFSP by radical radiotherapy (10, 11). Stereotactic radiosurgery is a technique that delivers a large ablative radiation dose to the tumour, without effect on the surrounding tissue. The Cyber Knife is a new, frameless stereotactic radiosurgery system, which consists of 3 key components: a lightweight linear accelerator (LINAC), a robotic arm that can point the LINAC from a wide variety of angles, and a tumour tracking system. This system is able to deliver extracranial stereotactic radiotherapy with millimetric precision, leading to disease control and toxicity profiles that are equal to or better than other radiotherapy techniques (12).
To our knowledge, there is no English-language report in which complete remission of DFSP without significant side-effects was achieved using Cyber Knife. Our present study suggests the novel possibility of using CyberKnife for the treatment of DFSP that is near a critical structure and for which standard surgical therapy with a wide margin is impractical, in addition to MMS. Since DFSP tends to recur long after the primary treatment and our follow-up period is short (13), further follow-up is needed for a definitive conclusion.
TThe authors declare no conflicts of interests.
References

