Yasumasa Shimasaki, Yukie Fukuta, Yuichi Yoshida*, Hiromi Higaki-Mori and Osamu Yamamoto
Division of Dermatology, Department of Medicine of Sensory and Motor Organs, Faculty of Medicine, 86 Nishi-cho, Yonago-shi, Tottori 683-8503, Japan. *E-mail: yxy@grape.med.tottori-u.ac.jp
Accepted May 9, 2012.
Agminated melanocytic naevi is a rare disorder characterized by grouped melanocytic lesions on a localized area of the body (1). Although agminated melanocytic naevi can be categorized into congenital and late-onset acquired types, acquired agminated melanocytic naevi is extremely rare (2–6). We report here two cases of acquired agminated melanocytic naevi and review the cases reported previously.
CASE REPORT
Case 1.
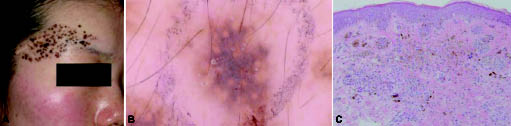
A 23-year-old Japanese woman was referred to our clinic with a pigmented lesion on the right side of her forehead. The pigmented spots had appeared at 4 years of age after a trauma. She had no family or past history of malignant melanoma. On physical examination, approximately 100 pigmented small macules were found in an 8 × 3.5 cm area on the right side of her forehead (Fig. 1A). There was a traumatic scar in the periphery of the lesion. On dermoscopic examination, typical pseudo-network was seen. No background pigmentation within the agminated lesion was noted (Fig. 1B). Histopathological examination showed naevus cell nests in both the basal layer of the epidermis and the dermis. Melanophages were also seen in the dermis. There was no apparent atypia in the naevus cells (Fig. 1C). Based on these findings, a diagnosis of acquired agminated melanocytic naevi (compound type) was made.
Fig. 1. (A) Agminated pigmented macules on the right side of the forehead. (B) Dermoscopic examination revealed typical pseudo-network. No background pigmentation was noted within the agminated lesion. (C) Naevus cell nests were seen both in the basal layer of the epidermis and in the dermis. There was no apparent atypia in the naevus cells (haematoxylin and eosin × 100).
Case 2
A 38-year-old Japanese woman was referred to our clinic with a pigmented lesion on her left forearm. The pigmented spots had appeared in her childhood. There was no history of trauma in the lesion. She had no family or past history of malignant melanoma. On physical examination, approximately 100 pigmented small macules were found in a 5 × 4 cm area on her left forearm (Fig. 2A). On dermoscopic examination, globular pattern was seen. No background pigmentation within the agminated lesion was noted (Fig. 2B). Histopathological examination showed elongation of the rete ridge and naevus cell nests in the epidermal basal layer. Many melanophages were also observed in the dermis. There was no apparent atypia in the naevus cells (Fig. 2C). Based on these findings, a diagnosis of acquired agminated melanocytic naevi (junctional type) was made.
Fig. 2. (A) Agminated pigmented macules were seen on the forearm. (B) On dermoscopic examination, globular pattern was seen. No background pigmentation was seen within the agminated lesion. (C) Naevus cell nests were seen in the basal layer of epidermis. There was no apparent atypia in the naevus cells (haematoxylin and eosin × 100).
DISCUSSION
Melanocytic tumours, such as melanocytic naevus (2–6), blue naevus (7) and Spitz naevus, (8) can occasionally appear as agminated lesions. In the present cases, the agminated macules dermoscopically lacked background pigmentation, unlike speckled lentiginous naevus. A diagnosis of agminated melanocytic naevi was made on the basis of clinical and histopathological examination. Although agminated melanocytic naevi can be categorized into congenital and acquired types, the distribution of congenital type is often segmental, following a dermatome or a Blaschko's line rather than "agminated". It has been assumed that the distribution is caused by a clonal outgrowth of cells originating from a somatic mutation at an early stage of embryogenesis (9). On the other hand, the pathogenesis of acquired type has not been elucidated. As far as we know, only 7 cases of acquired agminated melanocytic naevi (including the ones described here) have been reported in the English literature (2–6). Previously reported cases are summarized in Table I. We excluded cases of acquired agminated melanocytic naevi in association with dysplastic naevus syndrome because additional factors might be related to the pathogenesis. The mean age of the patients was 36.6 years. Onset age was less than 20 years in 6 cases. The site and number of naevi varied between cases, and 5 of the patients were female. Although 2 patients had a past history of a trauma within the lesion, the injury might be coincidental. We speculate that hormonal (growth) factors could be related to the pathogenesis of the disease. Histopathologically, there were various types (junctional, intradermal and compound type) of melanocytic naevi. However, it is notable that malignant melanoma developed from agminated lesions in 2 cases. Therefore, careful follow-up is recommended in patients with acquired agminated melanocytic naevi.
Table I. Cases of acquired agminated melanocytic naevi
|
Case no.
(age, years/sex)
|
Onset age (years)
|
Site
|
Naevi
n
|
Histopathology
|
Trauma
|
Author (ref)
|
|
1 (32/M)
|
After birth
|
Lower aspect of back
|
6
|
Not determined
|
Unknown
|
Bragg, et al. (2)
|
|
2 (36/F)
|
2
|
Right arm
|
Unknown
(>100?)
|
Melanoma
Compound naevi
|
Yes
(Burn)
|
Corradin, et al. (3)
|
|
3 (22/F)
|
17
|
Right sole
|
8
|
Junctional naevi
|
No
|
Tanioka, et al. (4)
|
|
4 (74/F)
|
74
|
Right breast
|
15
|
Compound naevi
|
No
|
Nakamura, et al. (5)
|
|
5 (32/M)
|
Teenage years
|
Left chest
|
50
|
Melanoma
Junctional naevi
Intradermal naevi
Compound naevi
|
No
|
Rezze, et al. (6)
|
|
6 (22/F)
|
4
|
Right forehead
|
100
|
Compound naevi
|
Yes
|
This report
|
|
7 (38/F)
|
Childhood
|
Left arm
|
100
|
Junctional naevi
|
No
|
This report
|
REFERENCES