


Taku Fujimura, Yumi Kambayashi, Takanori Hidaka, Akira Hashimoto, Takahiro Haga and Setsuya Aiba
Department of Dermatology, Tohoku University Graduate School of Medicine, Sendai, Japan
Regulatory T cells (Tregs), identified by the expression of CD4, CD25 and Foxp3, together with immunosuppressive macrophages, such as CD163+ M2 macrophages, are involved in maintaining peripheral tolerance. The aim of this study was to elucidate the involvement of Tregs and CD163+ macrophages in invasive and non-invasive extramammary Paget’s disease. The presence of CD4+CD25+Foxp3+ Tregs, CD163+ M2 macrophages and matrix metalloproteinase-9+ cells was examined immunohistologically in fixed sections of lesional skin from 10 patients with non-invasive extramammary Paget’s disease and 7 patients with invasive extramammary Paget’s disease. Fewer CD4+CD25+Foxp3+ Tregs were observed in non-invasive extramammary Paget’s disease than in invasive extramammary Paget’s disease. In contrast, higher numbers of CD163+ macrophages and metalloproteinase-9+ cells were detected only in invasive extramammary Paget’s disease. These findings suggest that the induction of immunosuppressive cells in extramammary Paget’s disease differs according to the tumour stage. Key words: regulatory T cells; Foxp3; CD163; macrophages; matrix metalloproteinase-9.
(Accepted June, 13, 2012.)
Acta Derm Venereol 2012; 92: XX–XX.
Taku Fujimura, Department of Dermatology, Tohoku University Graduate School of Medicine, Seiryo-machi 1-1, Aoba-ku, Sendai, 980-8574, Japan. E-mail: tfujimura1@mac.com
Immunological tolerance of self-antigens is essential for the prevention of autologous reactions and autoimmune diseases. In the peripheral organs, tolerance is reinforced by various mechanisms, including a population of regulatory T cells (Tregs) that actively suppress the function of autoreactive T cells. These Tregs are identified by the expression of Foxp3, CD4 and the IL-2Rα chain (CD25). Foxp3, a member of the forkhead family of transcription factors, is both necessary and sufficient for the development and function of those CD4+CD25+ Tregs (1).
The roles of Tregs are of interest in the field of human disease pathogenesis. Depletion of CD4+CD25+ Tregs results in the development of autoimmune disease and enhanced immune responses against alloantigens and tumour antigens (2, 3). Down-regulation of Tregs causes rejection of transplanted tumours by the host immune response (4). On the other hand, the high frequency of Tregs in patients with carcinomas reportedly contributes to lymphocyte dysfunction, leading to the suppression of anti-tumour immune responses (5). Tregs are thus inextricably connected with immune-tolerance and suppressed recognition of tumour antigens in tumour progression and recurrence. Together with Tregs, immunosuppressive macrophages, such as myeloid derived suppressor cells (MDSCs) and tumour-associated macrophages (TAMs), contribute to establishing the tumour microenvironment in skin cancer (6–8). In humans, tumour-associated macrophages are recognized as CD163+ M2 macrophages (7, 8).
Extramammary Paget’s disease (EMPD) is a skin adenocarcinoma that usually occurs in the anogenital region.Jang’s study of the prevalence of CD4+CD25+Foxp3+ Tregs in cutaneous squamous tumours (9) suggests that invasive skin cancer may be related to increased numbers of Tregs in the tumour lesion. Histologically, non-invasive EMPD and invasive EMPD show significant numbers of lymphocytes around the tumour mass.
The present study examined immunohistochemically the presence of Foxp3+ Tregs in the lesional skin of patients with non-invasive EMPD and those with invasive EMPD.
MATERIALS AND METHODS
Reagents
The following antibodies (Abs) were used for immunohistochemical staining: mouse monoclonal Abs for human CD3 and human CD4 (Nichirei Co., Tokyo, Japan), human CD8 (Dako A/S, Glostrop, Denmark), human CD25 (Vector, Burlingame, CA), human CD163 (Abcam, Tokyo, Japan), rabbit polyclonal Abs for human matrix metalloproteinase (MMP)-9 (Abcam), and rabbit anti-human Foxp3 Ab and immunoglobulin (Ig) from an unimmunized rabbit (BioLegend, San Diego, CA, USA). Mouse IgG1, IgG2b, and IgG2a isotype controls were obtained from R&D Systems (Minneapolis, MN, USA).
Immunohistochemistry for Foxp3 and CD3, CD4 or CD25
Archival formalin-fixed paraffin-embedded skin specimens from 10 patients with non-invasive EMPD and 7 patients with invasive EMPD treated in the Department of Dermatology at Tohoku University Graduate School of Medicine were collected. EMPD was defined by typical clinical and histological characteristics, such as Paget’s cells, defined as rounded cells devoid of intracellular bridges with a large nucleus and ample cytoplasm, present in the epidermis. Invasive EMPD is histologically defined as Paget’s cells infiltrated in the dermis. Immunohistochemical stainings for both invasive and non-invasive EMPD are cytokeratins 7+, cytokeratin 20–, periodic acid-Schiff (PAS)+ and Alcian blue stain (AB)+ in all cases. The 10 non-invasive EMPD samples and 7 invasive EMPD samples were processed for double staining of Foxp3 and CD3, CD4 or CD25, as described previously (10). Briefly, formalin-fixed paraffin-embedded tissue samples were sectioned at 4 µm and deparaffinized. After autoclaving for antigen retrieval treatment, the sections were blocked with goat serum for 10 min, then exposed to primary antibodies at 4ºC overnight. Antibody binding was demonstrated via alkaline phosphatase-conjugated anti-rabbit Ig (Histofine SAB-AP(R) kit; Nichirei Co.) for anti-Foxp3 Ab or immunoglobulin from an unimmunized rabbit, and via peroxidase-conjugated anti-mouse Ig (Histofine SAB-PO(M) kits; Nichirei) for the anti-CD3, anti-CD4, anti-CD25 Abs, or their isotype controls. Anti-Foxp3 Ab was developed with new fuchsin (Nichirei Co.), whereas the other mouse antibodies were visualized with 3,3’-diaminobenzidine tetrahydrochloride (Wako Pure Chemical Industries, Osaka, Japan).
Assessment of immunohistochemical staining
Staining of infiltrated lymphocytes was examined in more than 5 random, representative fields from each section. The number of immunoreactive cells was counted using a 1 cm2 ocular grid at a magnification of × 400. Treg cell fractions were defined as the ratio (%) of Foxp3+ cells among CD3+, CD4+ and CD25+ cell populations. Data are expressed as means ± standard deviations for Treg fractions in each skin disorder.
Statistical analysis
For a single comparison of 2 groups, Mann–Whitney U test was used. The level of significance was set at p = 0.05.
RESULTS
Foxp3+ T cells in invasive and non-invasive extramammary Paget’s disease
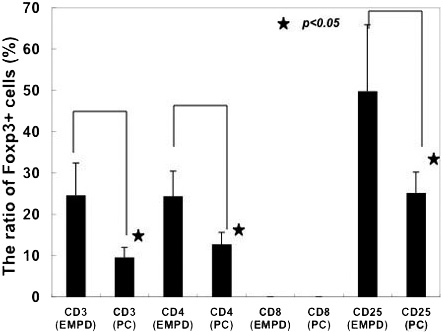
To evaluate the percentages of Foxp3+ cells among CD3+, CD4+ and CD25+ cell populations, immunohistochemical staining of Foxp3 together with CD3, CD4, CD8 or CD25 was performed in 10 samples from patients with non-invasive EMPD and 7 samples from patients with invasive EMPD. The antibody specificity to Foxp3 antigen using Foxp3-transfected cells (10) had been checked previously. Immunohistochemical staining showed infiltration of substantial numbers of Foxp3+ cells in the lesional skin of non-invasive EMPD (Fig. 1A, B) and invasive EMPD (Fig. 1C, D), but few Foxp3+ cells in normal skin (data not shown). The percentages of Foxp3+ cells in non-invasive EMPD and invasive EMPD were 24.6 ± 7.8% and 9.6 ± 2.4% among CD3+ cells, 24.4 ± 6.0% and 12.8 ± 2.8% among CD4+ cells, and 49.8 ± 16.1% and 25.2 ± 5.1% among CD25+ cells, respectively (Fig. 2). As reported previously, almost no Tregs are present in normal skin (10). The percentages of Foxp3+ cells among the CD3+, CD4+ and CD25+ populations were significantly higher in non-invasive EMPD than in invasive EMPD (p < 0.05).
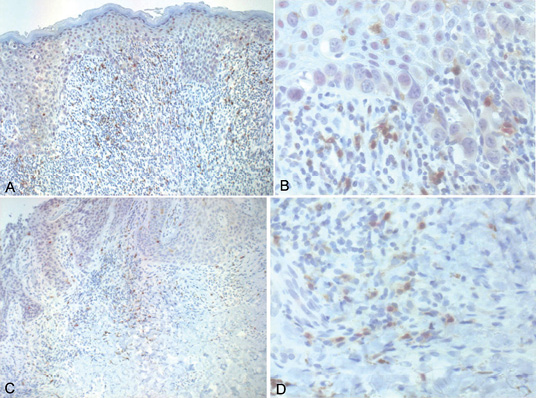
Fig. 1. Anti-Foxp3 antibody staining of non-invasive extramammary Paget’s disease (EMPD) and invasive EMPD. (A, B) Paraffin-embedded tissue samples from patients with non-invasive EMPD were deparaffinized and stained using a combination of the anti-Foxp3 Ab and an anti-CD25 Ab (A: ×100; B: ×400). (C, D) Paraffin-embedded tissue samples from patients with invasive EMPD were deparaffinized and stained with a combination of anti-Foxp3 Ab and anti-CD25 Ab (C: ×100; D: ×400). Sections were developed with new fuchsin for Foxp3 (red) and with 3,3'-diaminobenzidine tetrahydrochloride for CD25 (brown).
Fig. 2. Percentages of Foxp3+ cells among CD3+, CD4+, CD8+ or CD25+ T cells in lesional skin of non-invasive extramammary Paget’s disease (EMPD) and invasive EMPD. The Treg fraction was defined as the ratio (%) of CD3+Foxp3+, CD4+Foxp3+, CD8+Foxp3+ or CD25+Foxp3+ cells to the total number of CD3+, CD4+, CD8+ or CD25+ cells in each field, respectively. Data are expressed as means ± standard deviations of Treg fractions in each skin disorder. *p = 0.01. PC: Paget carcinoma; invasive EMPD.
CD163+ macrophages and MMP-9+ cells in invasive and non-invasive extramammary Paget’s disease
In order to examine the profiles of immunosuppressive cells around the tumour in invasive and non-invasive EMPD, we performed immunohistochemical staining of CD163 and MMP-9. In contrast to the tendency for Foxp3+ cell infiltration, few CD163+ cells or MMP-9+ cells were detected in non-invasive EMPD (Fig. 3A, B). In invasive EMPD, numerous CD163+ macrophages and MMP-9+ cells were detected around the tumour (Fig. 3C, D).
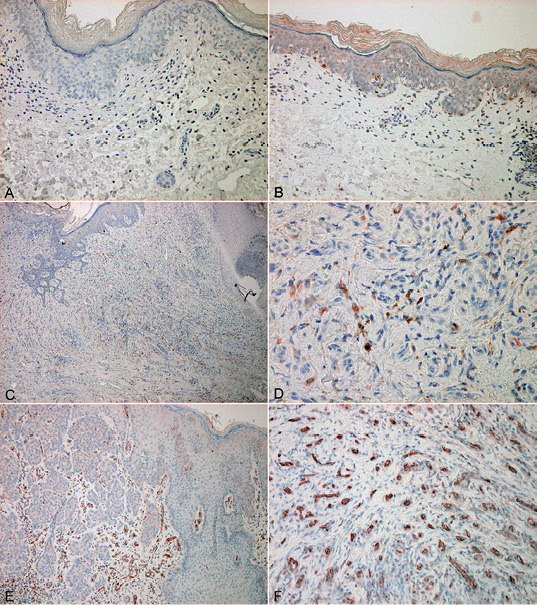
Fig. 3. Anti-CD163 and anti-MMP-9 antibody staining of non-invasive extramammary Paget’s disease (EMPD) and invasive EMPD. Paraffin-embedded tissue samples from patients with (A, B) non-invasive EMPD and (C, D, E, F) invasive EMPD were deparaffinized and stained using (A, C, D) anti-CD163 Ab or (B, E, F) an anti-MMP-9Ab (original magnification (C, E) ×100, (A, B) ×200, (D, F) ×400).
DISCUSSION
This study examined the compartmentalization of CD4+CD25+Foxp3+ Tregs and CD163+ macrophages in invasive and non-invasive EMPD. The results demonstrate the infiltration of numerous Foxp3+ Tregs around both types of tumour, and especially in invasive EMPD, and dense infiltration of CD163+ macrophages and MMP-9+ cells throughout the dermis. To the best of our knowledge, this represents the first quantitative analysis showing the percentages of Foxp3+ cells among infiltrating T cells in these kinds of skin tumours, together with CD163+ macrophages and MMP-9+ cells.
Quantitative analysis of the expression of Foxp3+ Tregs revealed that the populations of Tregs infiltrating non-invasive EMPD and invasive EMPD were accompanied by few or numerous CD163+ M2 macrophages and MMP-9+ cells, respectively. Press et al. (11) reported that increased Tregs may be associated with the recurrence of EMPD. In this respect, quantitative analysis of the expression of Foxp3+ Tregs in EMPD might be one of the crucial factors in assessment of the prognosis of EMPD. Together with other suppressor cells, such as MDSCs, TAMs and CD163+ M2 macrophages, Tregs promote an immunosuppressive environment in the tumour-bearing host (6–8, 12). In addition to directly suppressing effector T cells, Tregs also indirectly suppress effector T cells by several mechanisms through the suppression of antigen-presenting cells (APC): (i) suppression of the maturation of APC by interleukin (IL)-10; (ii) induction of APC apoptosis and reduction of the APC pool; (iii) increased production of kynurenines from APC; (iv) inhibition of APC activation via lymphocyte activation gene-3; (v) degradation of ATP into AMP by CD39 and the resultant abrogation of ATP-driven maturation of APCs (13); and (vi) increased expression of B7-homologue molecules (B7H3, B7H4) on APCs (12, 14). We have also shown that Tregs increased the expression of B7H1 on MDSCs in a melanoma model (15), and detected the expression of CD39 on Foxp3+ cells (Fig. S1; available from: http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1453), which suggests that infiltrating Foxp3+ cells may suppress the effector T cells in the tumour microenvironment by the degradation of ATP into adenosine. The increased level of Tregs in non-invasive EMPD and invasive EMPD suggests that Tregs not only directly suppress effector T cells against tumour cells, but also affect tumour stromal cells and maintain and induce immunosuppressive cells in the tumour microenvironment.
MMP-9 is a stromal factor that regulates the mobilization of hematopoietic stem cells from the bone marrow niche by solubilizing the membrane-bound form of c-KitL (16). Because it remodels the extracellular matrix and promotes the sprouting and growth of new blood vessels by making vascular endothelial growth factor (VEGF) available to the VEGFR-2/flk receptor on endothelial cells, MMP-9 is a lynchpin in tumour progression (16). Several reports have shown that expression of MMP-9 on tumours correlates with the progression or prognosis of several skin tumours, for example malignant melanoma, squamous cell carcinoma, basal cell carcinoma, mycosis fungoides, and angiosarcoma (16–21). In addition, other reports have indicated that the expression of MMP-9 on immunosuppressive macrophages in the tumour microenvironment contributes to tumour invasion and metastasis (6, 7, 21, 22). Taken together, these reports suggest that increased numbers of MMP-9+ cells around the tumour may be connected with CD163+ M2 macrophages and may contribute to the poor prognosis of invasive EMPD.
In the present study, the ratios of Foxp3+ cells among CD3+, CD4+ and CD25+ cells were found to be higher in non-invasive EMPD than in invasive EMPD. This discrepancy may be related to the facts that the expression of Foxp3 is induced in all CD4 T cells by antigenic stimulation (23), that the Foxp3+ CD4 T-cell fraction includes effector cytokine-producing, non-regulatory T cells (24), and that these non-regulatory Foxp3dull+ T cells are most probably effector T cells (25). Indeed, although we calculated the expression of Foxp3 only in highly expressed cells, the manual counting of immunoreactive cells may be a limitation of data collection in our study. In order to omit the mixing of effector T cells in our Foxp3+ cells, we also employed the immunohistochemical staining for CD39/ Foxp3 (Fig. S1). Although we did not investigate the concise profiles of effector T cells, if the effector T cells were also increased in invasive EMPD, the increase in immunosuppressive cells would be interpreted as a compensatory mechanism in the immune system. Since we did not directly assess the suppressive function of these infiltrating Tregs and M2 macrophages in this study, further analysis of the mechanisms underlying this phenomenon may offer fundamental insights into the mechanisms of invasive EMPD.
REFERENCES


