


Takamichi Ito1,2, Yuichi Yoshida1, Masutaka Furue2 and Osamu Yamamoto1
1Division of Dermatology, Department of Medicine of Sensory and Motor Organs, Faculty of Medicine, Tottori University, 36-1 Nishi-cho, Yonago-shi, Tottori 683-8503 and 2Department of Dermatology, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan. E-mail: takamiti@dermatol.med.kyushu-u.ac.jp
Accepted August 28, 2012.
Fibrous histiocytoma is a benign tumour composed of a mixture of fibroblastic and histiocytic cells and is one of the most common mesenchymal neoplasms of the skin (1, 2). Benign fibrous histiocytoma (BFH) most frequently occurs in the dermis and is rarely found in subcutaneous soft tissue, especially on the face. We present here for the first time a case of subcutaneous BFH showing nerve involvement in the eyebrow region.
CASE REPORT
A 42-year-old Japanese man was referred to our clinic with a 3-week history of a slow-growing subcutaneous mass on the left medial eyebrow region. Physical examination revealed a solitary, firm and well-demarcated subcutaneous tumour of 10 × 5 mm in size (Fig. 1). The mass was not adherent to the overlying skin. He complained of spontaneous pain and numbness on the left forehead. Past medical history and routine laboratory studies were unremarkable. A magnetic resonance imaging (MRI) scan demonstrated a well-circumscribed subcutaneous mass closely attached to the frontalis muscle. The mass showed isointensity on T1-weighted and hyperintensity on T2-weighted MR images. He underwent surgical excision of the mass under local anesthesia. Intraoperatively, the tumour was adherent to the frontalis muscle and involved the left supratrochlear nerve. Lateral margins of the tumour were not well-defined. Histopathologically, the tumour was lobulated but not encapsulated, showing ill-defined margins. The tumour had infiltrated into surrounding muscle at the periphery. A large nerve was involved in the lesion. The tumour was composed of bland ovoid-to-spindle cells arranged in a storiform pattern admixed with lymphocytes. Several multinucleate giant cells were observed. There were a few mitoses (2~3/HPF), but no abnormal mitoses were found (Fig. 2). Immunohistochemically, more than half of tumour cells were positive for Factor XIIIa, but the tumour cells were negative for CD34, making dermatofibrosarcoma protuberans unlikely, and S-100 protein. Based on these findings, a diagnosis of subcutaneous BFH was made. His postoperative course was uneventful apart from residual numbness on the left forehead.

Fig. 1. A solitary, firm and well-demarcated subcutaneous tumour is observed on the left medial eyebrow region.
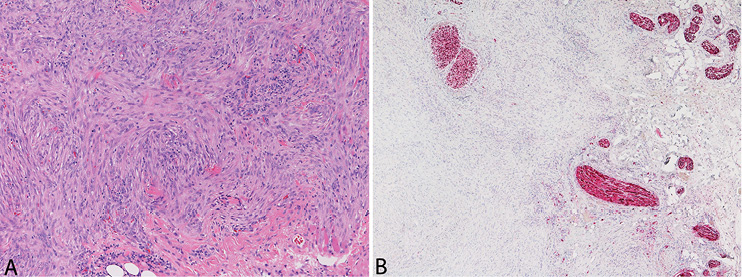
Fig. 2. The tumour is composed of bland ovoid-to-spindle cells arranged in a storiform pattern (HE staining, × 100) (A). A large nerve is involved in the lesion (immunohistochemical staining for S-100 protein, × 40) (B).
DISCUSSION
BFH usually arises in the skin, which is referred to as dermatofibroma but occurs in subcutaneous or deep soft tissue in only about 1% of all BFH (3, 4). Similar to cutaneous BHF, subcutaneous or deep BFH presents over a broad age range and is most common on the extremities (2). Subcutaneous BHF occurring on the face is extremely rare. To our knowledge, only 12 cases have been reported to date and the present case is the first case occurring on the eyebrow region (2, 3, 5, 6).
Subcutaneous or deep BFH has a higher risk of local recurrence than that of cutaneous BFH. Gleason & Fletcher. (2) reported that the local recurrence rate of deep BFH was 22%. The rate is significantly higher than that of conventional cutaneous BFH but is similar to that of other clinically aggressive subtypes such as cellular, aneurysmal and atypical variants of cutaneous fibrous histiocytoma. In addition, BFH in the face, even cutaneous type, recurs more frequently than does BFH in other regions such as the extremities, corresponding to the other above-mentioned subtypes (cellular, aneurysmal and atypical variants) (7). The high recurrence rate can be explained by diffuse infiltration into deeper structures and incomplete excision due to the anatomical characteristics.
It is noteworthy that our patient complained of spontaneous pain and numbness of the left forehead preoperatively. We suspected that the tumour was a nerve-derived tumour such as schwannoma because of the finding of supratrochlear nerve involvement in the mass during surgery. Although BFH usually does not evoke subjective symptoms, it occasionally shows infiltration of subcutaneous and deep soft tissue (1, 7). In our case, it is likely that the spontaneous pain and numbness on the forehead were caused by tumour involvement of the supratrochlear nerve. When excising a subcutaneous tumour on the face, surgeons should be aware of the possibility that the tumour may be a BFH involving important surrounding nerves and vessels.
The authors declare no conflicts of interest.
REFERENCES

