


Unilateral Eruption of Painful Papules: A Quiz
Annabel D. Scott, Nicholas Francis and Sarita Singh
Department of Dermatology, Chelsea and Westminster Hospital, SW10 9NH London, United Kingdom. E-mail: annabel.scott@doctors.org.uk
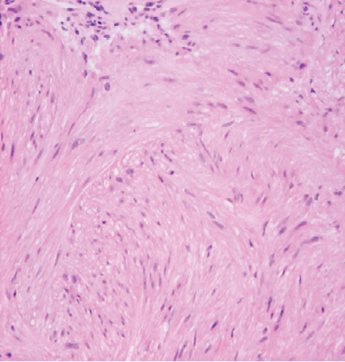
A 36-year-old man of Pakistani origin presented with a 10-year-history of unilateral lesions involving his left arm, left torso and left leg. The lesions were painful following showers and on light touch. He was otherwise well with no significant past medical history. There was no family history of similar lesions and his parents were non-consanguineous. On examination, groups of firm reddish brown papules were seen over the left hand side of the body (Fig. 1). The lesions did not cross the midline. On histological examination of a lesional punch biopsy, a dermal tumour consisting of densely arranged interlacing fascicles of spindle cells with blunt ended nuclei and eosinophilic cytoplasm was seen. There was no pleomorphism or mitotic activity (Fig. 2).
Fig. 1. Groups of erythematous reddish brown papules on the trunk.

Fig. 2. Spindle cells with blunt ended nuclei.
What is your diagnosis? See next page for answer.
doi: 10.2340/00015555-1774
Unilateral Eruption of Painful Papules: A Comment
Acta Derm Venereol
Diagnosis: Type 1 Segmental Cutaneous Leiomyomatosis
Cutaneous leiomyomas, also known as pilar leiomyomas, are benign tumours arising from the arrector pili muscle of the hair follicle. In over 80% of cases multiple lesions occur simultaneously in either a disseminated or segmental pattern (1). Cutaneous leiomyomas in women may be associated with uterine leiomyomas, when the condition is then termed multiple cutaneous and uterine leiomyomatosis (MCUL). Hereditary leiomyomatosis, and renal cell carcinoma (HLRCC) is a disease variant where patients present with aggressive renal cell carcinomas. It has recently been demonstrated that patients with MCUL and HLRCC have a germline mutation in one copy of the gene encoding the enzyme fumarate hydratase (2).
Woyska first described a segmental form of multiple cutaneous leiomyomas in 1934 (3). There have been at least 9 case reports since. Happle (4) noted that autosomal disorders can present in a segmental fashion and categorised segmental presentations as types 1 and 2. Type 1 distributions are due to mosaicism whereby a post-zygotic mutation leads to the development of the disorder within the lines of Blaschko. The patient does not have a family history of the disorder and lesions are not seen elsewhere on the body (3). In a type 2 segmental presentation a heterozygote embryo undergoes a post-zygotic loss of heterozygosity, thereby leading to a more pronounced presentation of the disorder within the lines of Blaschko as well as the normal non-mosaic phenotype elsewhere. These patients usually have a family history of the disorder (3). Cutaneous leiomyomatosis has more frequently been reported as presenting in a type 2 distribution (4).
Given that our patient has no family history of cutaneous leiomyomas, presented later in life and with unilateral lesions we propose that our patient has a type 1 presentation. There is only one other case report of a type 1 presentation of segmental cutaneous leiomyomas (5).
The aim of treatment of this disorder is to relieve pain; although the pathogenesis of pain-associated cutaneous leiomyomas is uncertain. Various theories have been proposed including pressure on nerve fibres and abnormal erector pili muscle contraction. Carbon dioxide laser ablation, hyoscine butyl bromide, nifedipine, phenoxybenzamine, doxazosin, and gabapentin have all been tried with varying degrees of success (6).
References

