


Sarah C. Wallingford1, Sheila A. Russell2, Andy Vail3, Charlotte M. Proby4, John T. Lear1,5 and Adèle C. Green1,6
1Institute of Inflammation and Repair, University of Manchester, Manchester Academic Health Sciences Centre, 2Kidney and Pancreas Transplant Unit, Manchester Royal Infirmary, Manchester, 3Centre for Biostatistics, University of Manchester, Manchester Academic Health Sciences Centre, Salford Royal Hospital, Salford, 4Division of Cancer Research, Medical Research Institute, Ninewells Hospital and Medical School, Dundee, 5Department of Dermatology, Manchester Royal Infirmary, Manchester, UK, and 6Cancer & Population Studies Group, QIMR Berghofer Medical Research Institute, Brisbane, Australia
While actinic keratoses (AKs) have a known association with cutaneous squamous cell carcinoma (SCC), the relation of actinic field change to SCC has not been quantified. This study investigated the presence of field change and AKs in renal transplant recipients (RTRs) and estimated SCC risk. In May 2010 to October 2011, a dermatologist examined 452 white RTRs (mean age 53 years) at two hospitals in Manchester, UK, counting AKs and recording field change presence by body site and SCCs arising during the study period. Of the participants 130 (29%) had AKs at examination. In 60 (13%) RTR patients with AKs but no field change, 4 (7%) developed SCCs, compared with 15 (21%) of the 70 (15%) with AKs and field change. SCCs developed directly within field change areas in 11/15 (73%) RTRs. This study confirms that RTRs with widespread confluent actinic skin damage are at very high risk of SCC and should be monitored closely. Key words: actinic keratosis; actinic field change; renal transplant recipients; squamous cell carcinoma; immunosuppression.
Accepted Mar 17, 2015; Epub ahead of print Mar 18, 2015
Acta Derm Venereol
Adèle C. Green, Cancer Research UK Manchester Institute, University of Manchester, Wilmslow Road, Manchester M20 4BX, UK. E-mail: adele.green@cruk.manchester.ac.uk
Renal transplant recipients (RTRs) are at increased risk of keratinocyte cancers, namely cutaneous squamous cell carcinomas (SCCs) and basal cell carcinomas (BCCs), as a result of their immunosuppressive therapy (1–3). They also have a greatly elevated risk of developing associated benign and premalignant lesions, the most common being actinic keratoses (AKs) as well as numerous dysplastic warty lesions and verrucous keratoses (4). The prevalence of all such lesions rises with increasing duration of immunosuppression (3, 5, 6). AKs are important not only as risk indicators of BCC and SCC occurrence (4, 7), but also because a small proportion progress to invasive SCCs. The overall transformation rate of a single AK to SCC has been estimated at between 0% to 0.075% per year and up to 0.53% in people with a history of skin cancer (8).
As AKs become very numerous on a given anatomic site, they frequently appear as confluent fields of actinic damage, known as actinic field change or field cancerisation (9, 10). Within these areas the skin is not only clinically abnormal but also histologically dysplastic (11–13). Given the molecular evidence that field damage presages carcinogenesis (14), cutaneous field change is thus believed to carry a heightened risk of SCC (3). Previous studies have often failed to evaluate actinic field change however, or where confluent lesions are present, AK counts have been said to be ‘indeterminate’ (15). Consequently, little evidence is available about determinants of actinic field change or the actual magnitude of its association with SCC.
In this study we assessed the prevalence of field change as well as of AKs in a large series of RTRs in Manchester, UK. We also examined risk factors for actinic field change and quantified the risk of developing SCC in the short to medium term.
Materials and Methods
Study population
The study population comprised white RTRs attending dermatological clinics at two tertiary hospitals in Greater Manchester for routine follow-up between May 2010 and October 2011. All RTRs in Manchester are referred to these clinics 12 months after transplantation for full skin assessment and ongoing routine follow-up (3). Inclusion criteria for this study were RTRs aged 18 or older with a currently functioning allograft, whose transplant surgery was at least one year prior to study enrolment. Only white Caucasian RTRs were eligible since the risk of skin cancer among non-white individuals is very low (16). Written informed consent was obtained from all participants and the study was approved by the North West 6 Research Ethics Committee, Greater Manchester South.
Data collection
On recruitment all patients were interviewed using a structured questionnaire to collect demographic information, details of sun sensitivity and occupational sun exposure and smoking history. Participants underwent full-body skin either by a single nurse with specialist dermatology training and 15 years’ experience in dermatologic assessment who screened patients’ skin for lesions, or by a consultant dermatologist who examined those with any actinic lesions. AKs were defined as discrete erythematous lesions with scaling and were counted and recorded by body site (including keratoses with warty features) (17). Areas of merging AKs, defined as areas of skin greater than 1 cm2 with confluent erythema and scaling, were also identified and recorded by site. For the purposes of this study we have called these areas actinic field change. For logistic reasons neither precise surface area measurements nor histological assessments of actinic field change could be routinely carried out in this study, however majority of participants had areas less than a single functional unit (e.g., dorsal hand, arm, forehead, scalp, etc). A standard protocol for quantifying AK and field change was developed separately (17) and many AK lesions observed in the clinic populations from which we obtained our participants were confirmed after biopsy or excision during routine dermatologic surveillance. The presence of viral warts (filiform lesions with no erythema) was also noted. All lesions suspicious for keratinocyte cancers were biopsied. Photographic examples of the different types of keratotic lesions identified in this study are provided in Fig. 1.
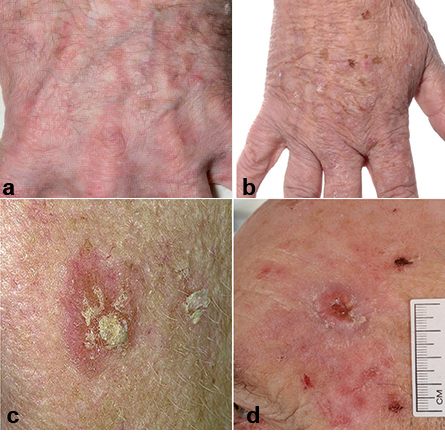
Fig. 1. Examples of the spectrum of keratotic lesions encountered in the renal transplant study population from Manchester, UK: a) discrete actinic keratoses (AKs), b) verrucous (warty) keratoses,c) discrete AKs nearly merging into a confluent area, and d) squamous cell carcinoma arising in area of confluent AKs.
Participants’ hospital records were examined to obtain detailed clinical information about history of renal transplantation, current immunosuppressive drug regimen and prescribed aspirin use post-transplant. In addition, histology and exact site of all confirmed skin cancers diagnosed and treated during the study period were obtained from surgical and histopathology records.
Analyses
Multi-factorial logistic regression was used to determine risk of AKs with and without actinic field change, adjusting for sex and age at examination, hospital site and duration of immunosuppression. Odds ratios (OR) with 95% confidence intervals (CI) for each risk factor were assessed. For all patients with field change who developed SCC during the study period, the study dermatologist noted whether or not the precise site of the SCC had occurred within an area of prevalent field change. Odds of SCC in relation to AKs without and with field change were also calculated, controlling for the same risk factors. All analyses were performed using SAS version 9.3 (Cary, North Carolina, USA). Significance was set at p < 0.05.
Results
Patient characteristics
Of 360 RTRs approached at the first Manchester renal transplant dermatology clinic, 10 outright refused participation at first approach and 24 elected not to provide written consent after familiarisation with the study information sheet, leaving 326 (91%) participants from that clinic, while all 126 RTRs approached at the second clinic consented to take part. Thus of 486 eligible RTRs attending dermatologic follow-up in Manchester, 452 (93%) patients were included in analyses. Participants from the first clinic were significantly younger at transplant than those from the second (mean age 41 versus 46 years), and consequently the former had a longer mean duration of immunosuppression (12 versus 9 years), but otherwise participants from the two hospitals were similar. Overall mean age of participants at time of skin examination was 53 years (range 18–84 years) and overall mean duration of immunosuppression was 11 years (range 1–41 years) with 15% having received more than one allograft. During the study period 36 (8%) RTRs were diagnosed with BCC and 20 (4%) with SCC (Table I). Patients were receiving a range of immunosuppressants, alone or in combination, namely ciclosporin (n = 117), azathioprine (n = 112), prednisolone (n = 239), tacrolimus (n = 237), mycophenolic acid/mycophenolate mofetil (n = 153) and 15 (3%) were being treated with sirolimus.
Prevalence of AKs and field change
One hundred and thirty (29%) RTRs had AK lesions present at skin examination, of whom 93 (72%) had AKs on more than one site, mostly on the head/neck (85%) and arms/hands (78%). Of the 130 with AKs, 58 (45%) had AKs only and 70 (54%) also had actinic field change (no patient had field change without AKs also present, notwithstanding 2 patients with unknown field change). In relation to duration of immunosuppression, 13% of RTRs with AKs without visible field change had been immunosuppressed for 20 or more years compared with 57% of those with field change present (p < 0.05) (Table I). Furthermore, 21% RTRs with field change had been immunosuppressed for 30 years or longer, compared with 3% of those with AKs without field change.
Table I. Characteristics of renal transplant recipients with actinic keratoses (AKs) only and with AKs and field change
|
Participant characteristics |
All (n = 452) n (%) |
AKs only (n = 58) n (%) |
AKs with field change (n = 70) n (%) |
|
Sex |
|
|
|
|
Male |
287 (63) |
34 (59) |
57 (81) |
|
Female |
165 (37) |
24 (41) |
13 (19) |
|
Age at examination |
|
|
|
|
18–39 years |
63 (14) |
1 (2) |
– |
|
40–59 years |
237 (52) |
25 (36) |
30 (43) |
|
≥ 60 years |
152 (34) |
32 (55) |
40 (57) |
|
Age at first transplant |
|
||
|
< 20 years |
37 (8) |
1 (2) |
10 (14) |
|
20–39 years |
170 (38) |
16 (28) |
25 (36) |
|
40–59 years |
186 (41) |
27 (47) |
25 (36) |
|
≥ 60 years |
59 (13) |
14 (24) |
10 (14) |
|
Duration of immunosuppression |
|||
|
< 10 years |
236 (52) |
29 (50) |
17 (24) |
|
10–19 years |
138 (31) |
21 (36) |
13 (19) |
|
20–29 years |
59 (13) |
6 (10) |
25 (36) |
|
≥ 30 years |
19 (4) |
2 (3) |
15 (21) |
|
Skin type |
|
||
|
Always burns/never tans |
70 (15) |
15 (26) |
14 (20) |
|
Usually burns/tans a little |
179 (40) |
25 (43) |
31 (44) |
|
Burns rarely/tans gradually |
156 (35) |
16 (28) |
17 (24) |
|
Never burns/always tans |
43 (10) |
2 (3) |
6 (9) |
|
Pre-transplant occupational sun exposure |
|||
|
Mainly indoor |
284 (63) |
36 (62) |
38 (54) |
|
Mixed |
65 (14) |
9 (16) |
12 (17) |
|
Mainly outdoor |
62 (14) |
8 (14) |
13 (19) |
|
Not employed |
34 (8) |
3 (5) |
3 (4) |
|
Post-transplant occupational sun exposure |
|||
|
Mainly indoor |
231 (51) |
26 (45) |
34 (49) |
|
Mixed |
40 (9) |
3 (5) |
8 (11) |
|
Mainly outdoor |
34 (8) |
3 (5) |
11 (16) |
|
Not employed |
138 (31) |
24 (41) |
13 (19) |
|
Smoking status |
|
||
|
Never |
258 (57) |
31 (53) |
40 (57) |
|
Ever |
187 (41) |
26 (45) |
26 (37) |
|
< 20 pack-years |
132 (29) |
17 (29) |
19 (27) |
|
≥ 20 pack-years |
46 (10) |
8 (14) |
5 (7) |
|
Prescribed aspirin post-transplant |
|||
|
No |
187 (41) |
18 (31) |
36 (51) |
|
Yes |
262 (58) |
40 (69) |
32 (46) |
|
Viral warts at examination |
|
||
|
Absent |
333 (74) |
30 (52) |
19 (27) |
|
Present |
103 (23) |
24 (41) |
48 (69) |
|
BCC diagnosed during study period |
|||
|
No |
414 (92) |
45 (78) |
54 (77) |
|
Yes |
36 (8) |
12 (21) |
15 (21) |
|
SCC diagnosed during study period |
|||
|
No |
430 (95) |
53 (91) |
54 (77) |
|
Yes |
20 (4) |
4 (7) |
15 (21) |
BCC: basal cell carcinoma; SCC: squamous cell carcinoma.
Of 130 RTRs with AKs, 62 had between 1 and 9 lesions, of whom 9 (7%) also had actinic field change (Fig. 2). Of the 68 (52%) RTRs who presented with 10 or more AKs (to a maximum lesion count of 69), 61 (89%) had concurrent field change.
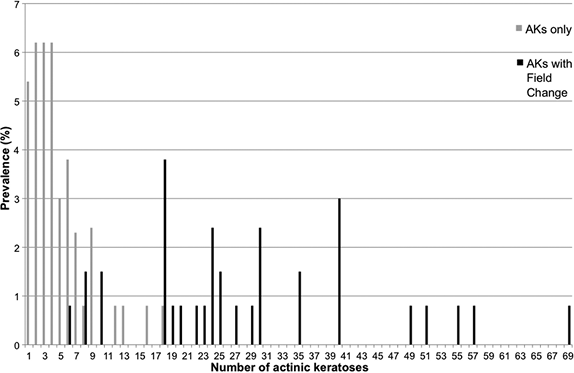
Fig. 2. Prevalence of total number of actinic keratoses (AKs) by field change status.
Risk factors
Characteristics of patients with AKs with and without actinic field change tended to be comparable in comparison with the characteristics of all RTRs in the study (Table I). On multi-factorial analyses controlling for sex, age at examination, hospital and duration of immunosuppression, RTRs with skin which always burns/never tans had 6-fold higher odds (OR 6.2, 95% CI 1.2, 31) of having AKs compared to those who never burnt and always tanned and RTRs with viral warts had significantly higher odds of concurrent AKs and field change compared to those without warts (Table II). There was no association with other factors including occupational sun exposure, smoking and prescribed aspirin use after adjustment of confounding factors.
Table II. Risk factors associated with actinic keratoses (AKs) only and AKs with actinic field change, compared to no AK
|
Patient characteristics |
AKs only OR (95% CI)a |
AKs with field change OR (95% CI)a |
|
Skin type |
|
|
|
Always burns/never tans |
6.2 (1.2, 31) |
1.6 (0.40, 6.4) |
|
Usually burns/tans a little |
4.6 (0.98, 22) |
1.3 (0.39, 4.4) |
|
Burns rarely/tans gradually |
2.3 (0.48, 11) |
0.47 (0.13, 1.7) |
|
Never burns/always tans |
1.0 |
1.0 |
|
Post-transplant occupational sun exposure |
||
|
Mainly indoor |
1.0 |
1.0 |
|
Mixed |
0.57 (0.15, 2.1) |
1.1 (0.38, 3.5) |
|
Mainly outdoor |
0.74 (0.19, 3.0) |
1.4 (0.42, 4.4) |
|
Not employed |
1.0 (0.51, 2.2) |
0.58 (0.23, 1.5) |
|
Smoking status |
|
|
|
Never |
1.0 |
1.0 |
|
Ever |
1.0 (0.54, 1.8) |
0.74 (0.35, 1.5) |
|
Took aspirin post-transplant |
||
|
No |
1.0 |
1.0 |
|
Yes |
1.5 (0.76, 2.9) |
0.91 (0.44, 1.9) |
|
Viral warts at examination |
|
|
|
Absent |
1.0 |
1.0 |
|
Present |
8.1 (3.8, 17) |
20 (7.8, 49) |
aAdjusted for sex, age at examination, hospital clinic attended and duration of immunosuppression.
OR: odds ratio; CI: confidence intervall.
Table II. Risk factors associated with actinic keratoses (AKs) only and AKs with actinic field change, compared to no AK
|
Patient characteristics |
AKs only OR (95% CI)a |
AKs with field change OR (95% CI)a |
|
Skin type |
|
|
|
Always burns/never tans |
6.2 (1.2, 31) |
1.6 (0.40, 6.4) |
|
Usually burns/tans a little |
4.6 (0.98, 22) |
1.3 (0.39, 4.4) |
|
Burns rarely/tans gradually |
2.3 (0.48, 11) |
0.47 (0.13, 1.7) |
|
Never burns/always tans |
1.0 |
1.0 |
|
Post-transplant occupational sun exposure |
||
|
Mainly indoor |
1.0 |
1.0 |
|
Mixed |
0.57 (0.15, 2.1) |
1.1 (0.38, 3.5) |
|
Mainly outdoor |
0.74 (0.19, 3.0) |
1.4 (0.42, 4.4) |
|
Not employed |
1.0 (0.51, 2.2) |
0.58 (0.23, 1.5) |
|
Smoking status |
|
|
|
Never |
1.0 |
1.0 |
|
Ever |
1.0 (0.54, 1.8) |
0.74 (0.35, 1.5) |
|
Took aspirin post-transplant |
||
|
No |
1.0 |
1.0 |
|
Yes |
1.5 (0.76, 2.9) |
0.91 (0.44, 1.9) |
|
Viral warts at examination |
|
|
|
Absent |
1.0 |
1.0 |
|
Present |
8.1 (3.8, 17) |
20 (7.8, 49) |
aAdjusted for sex, age at examination, hospital clinic attended and duration of immunosuppression.
OR: odds ratio; CI: confidence intervall.
Actinic keratosis and field change status and squamous cell carcinoma occurrence
The risk of SCC was significantly increased in the 15 (21%) RTRs with AKs and field change (OR 93; 95% CI 9.7, 890) and higher than the corresponding risk of SCC in the 4 (7%) RTRs with AKs but no field change (OR 20; 95% CI 2.1, 195), compared with the one person with SCC but no prevalent keratotic lesions. Of 20 RTRs with SCCs diagnosed in the study period, 11 (55%) developed the malignancy directly in an area of field change. The predominant site for SCC in an area of field change was the scalp (n = 5) followed by the face (n = 3). One RTR developed two SCCs in areas of field change on two different sites.
Discussion
We have documented the prevalence of actinic field change in relation to AKs in a cohort of RTRs and estimated the odds of developing SCC when visible widespread actinic damage is present, neither of which have been quantified previously. Overall in the Manchester RTR study population of mean age 53 and with mean duration of immunosuppression 11 years, 15% had actinic field change as well as AKs present and 14% had AKs present without field change. We estimate that in the short to medium term, SCCs are around 4 times more likely to develop in RTRs who have confluent areas of actinic damage than in those with AKs but without field change (3).
Our overall estimated AK prevalence in a contemporary RTR population is higher than reports of 11% and 15% prevalence observed in other UK-based studies of transplant populations (6, 18) several decades ago. On the other hand the increased risk of SCC associated with AKs is well-established (8) and the even greater SCC risk in the presence of field change has been suspected before if not quantified (3, 14). This is consistent with the observation that risk of SCC increases as the number of keratotic lesions increases (4, 19, 20).
There are many important risk factors for both AK and SCC in RTRs including sex, skin type, duration of immunosuppression, age at transplant and sun exposure (3–5, 21) as well as less established factors such as viral warts and infection with human papillomavirus (22). Accordingly we explored many of these in relation to AKs without and with field change and confirmed the well-established clinical observation of higher prevalence of AKs with longer duration of immunosuppression (5, 6). We further showed that, as expected, those immunosuppressed for 20 or more years were much more likely to have actinic field change than those with shorter durations of immunosuppression. The strong association seen between viral warts and AKs, with or without field change, reflects the increased likelihood of prevalent viral warts in patients with increasing duration of immunosuppression (4). Contrary to other reports we found that older age at transplant reduced the odds of AKs with and without field change, and believe this is because the majority of older patients in our study had only recently been transplanted, reflecting contemporary clinical practice. The predominance of AKs and particularly field change on highly-exposed body sites of RTRs (i.e. head and upper limbs) was also compatible with previous observations in other transplant populations (19, 23, 24).
Besides its novelty in showing the clinical relevance of systematically documenting actinic field change as well as AKs, the main strengths of this study were its capture of a largely representative population of RTRs in northwest England, all of whom received expert dermatologic examinations. Limitations of the study include the lack of information of past AKs and exact timing of first appearance of field change since a small number of RTRs in the study had SCC diagnosed within the defined study period but shortly before the study skin examination. Given the chronic nature of coalesced actinic keratotic damage and its development over many years, it is reasonable to assume it was present at the outset of the 18 months study period, well before the diagnosis of SCC. Other limitations were the lack of surface area measurements of the coalesced actinic keratotic damage in affected patients (not feasible for the dermatologist during the routine clinics) and lack of knowledge of participants’ history of skin cancer prior to immunosuppression, and thus neither of these likely important factors could be accounted for in analyses of SCC risk. Finally the relatively few RTRs who developed SCCs in the study period meant that our estimates were lacking in precision.
In conclusion, we have provided new evidence that the presence of areas of severe actinic skin damage in addition to the presence of AKs in RTRs confers an even higher risk of SCC than seen in RTRs with AKs but no such field of damage. Long-standing transplant recipients with clinical signs of actinic field change warrant close surveillance for skin cancer.
Acknowledgements
We are indebted to the participants of the study for their contribution. Thank you also to Mr. Christopher G. Duff, consultant plastic surgeon at the University Hospital of South Manchester, Manchester, UK for his assistance with clinical data checking. SC Wallingford and AC Green were supported in part by a fellowship from the Medical Research Council, UK (grant number 89912).
The authors declare no conflicts of interest.
References

