


Yukari Ise1, Yasushi Suga1, Kazuko Okumura1, Osamu Negi1, Norito Ishii2 and Takashi Hashimoto3*
1Department of Dermatology, Juntendo Urayasu Hospital, Urayasu, Chiba, 2Department of Dermatology, Kurume University School of Medicine, and 3Kurume University Institute of Cutaneous Cell Biology, 67 Asahimachi, Kurume, Fukuoka, Japan. *E-mail: hashimot@med.kurume-u.ac.jp
Accepted Sep 30, 2015; Epub ahead of print Oct 6, 2015
There are a number of variants of bullous pemphigoid (BP), including nodular pemphigoid, pemphigoid vegetans, lichen planus pemphigoides and dyshidrosiform pemphigoid (1). In addition, a few patients show erythema annulare centrifugum-like, erythema multiforme-like and erythema gyratum repens-like lesions (1). Cases showing annular erythemas without extensive blister formation can collectively be classified as erythematous variety of BP (2).
The association of BP with internal malignancy is a matter of debate, although some large retrospective studies have indicated a slight association (3). Indeed, some patients with BP have erythema gyratum repens-like clinical features.
We present here a case of erythematous variety of BP with no apparent internal malignancy.
CASE REPORT
In November 2012, an 81-year-old Japanese male developed pruritic erythemas on his entire body, which enlarged in an annular configuration. The skin lesions did not respond to topical corticosteroid and anti-histamine therapy. The patient had no particular family history, but was taking nifedipine and isosorbide mononitrate for ischaemic heart disease and tamsulosin hydrochloride and oxybutynin hydrochloride for benign prostatic hypertrophy. However, there was no definite evidence suggesting that these drugs triggered the erythematous skin lesions in this patient.
Physical examination revealed multiple exudative annular erythemas on the trunk and extremities (Fig. 1a,b). A healing tendency with slight pigmentation was seen in the centre of the erythema (Fig. 1c). No blister formation was seen. There were no oral or ocular mucosal lesions. No abnormal finding was shown in extensive laboratory studies, including routine blood tests and urinalysis, serum levels of complement components and various anti-nuclear autoantibodies.
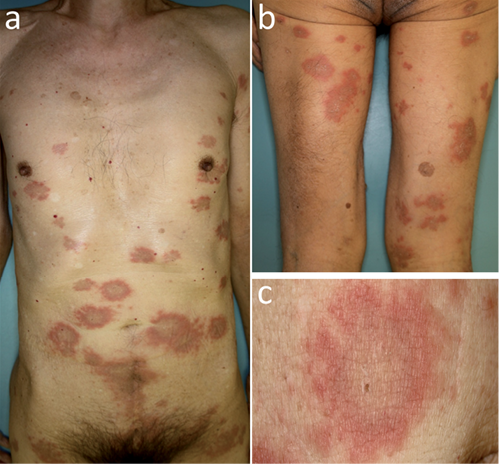
Fig. 1. Clinical features at the first visit. (a,b) Annular erythematous skin lesions with no blisters on (a) the abdomen and (b) the thighs. (c) Higher magnification of an annular erythema.
Histopathology of a skin biopsy from an erythematous lesion on the waist showed interface dermatitis with eosinophilic infiltration, but no subepidermal blistering (Fig. 2a). Direct immunofluorescence (IF) revealed linear deposition of immunoglobulin G (IgG) and C3 in the epidermal basement membrane zone (Fig. 2b).

Fig. 2. (a) Histopathological features. (b) Direct immunofluorescence for immunoglobulin G (IgG) deposition. (c) Indirect immunofluorescence of 1M NaCl-split-skin for IgG antibodies. Original magnification (a–c): × 400.
Indirect IF of normal human skin showed negative results, while indirect IF of 1M NaCl-split-skin showed IgG reactivity with epidermal side of the split at a titre of 1:20 (Fig. 2c). Complement IF of both normal human skin and 1M NaCl-split-skin showed negative results, suggesting that anti-basement membrane zone antibodies in the patient serum had low complement activation ability.
Enzyme-linked immunosorbent assays (ELISAs) (MBL, Nagoya, Japan) showed a positive result for BP180 (index 74, cut-off <9), but negative result for BP230 (index <5, cut-off <12). However, no positive results were detected in immunoblot analyses of various antigen sources, including normal human epidermal and dermal extracts, recombinant proteins of BP180 NC16a and C-terminal domains, concentrated culture supernatant of HaCaT cells and purified human laminin-332.
As differential diagnoses, we considered erythema exsudativum multiforme, erythema annulare centrifugum, annular erythema associated with Sjögren’s syndrome, rheumatic annular erythema, subacute cutaneous lupus erythematosus and dermatitis herpetiformis Duhring. To exclude these diseases, we performed various tests, including levels of complement components, anti-nuclear antibodies and autoantibodies to Ro, La and dsDNA, all with negative results. Therefore, we diagnosed this case as erythematous variety of BP.
Oral prednisolone, 10 mg/day, with oral fexofenadine, 120 mg/day, and topical dexamethasone propionate was not effective. However, after addition of a combination of roxithromycin, 300 mg/day, and niacinamide, 900 mg/day, the skin lesions disappeared within 2 weeks. The patient was free from any skin lesions on niacinamide, 900 mg/day, 2 years after initiation of therapy.
No internal malignancy was detected despite extensive examination, including various imaging and endoscopic examinations, performed during admission. No internal malignancy was found during the 2-year follow-up period.
Literature review for erythematous variety of BP
We searched the literature in English and Japanese and gathered 15 cases, including the present case, diagnosed as erythematous variety of BP (Table SI1) (4–14). There were 7 males and 8 females, age range 45–84 years (mean age 70.73 years). Only one of the 14 previous cases and our case exclusively showed erythemas; the other 13 patients developed bullous skin lesions, either simultaneously or later.
Among the 15 cases, 4 had internal malignancy, with one case each of rectal adenocarcinoma, colon cancer, lung cancer and breast cancer. In the patient associated with colon cancer the annular erythemas disappeared significantly after removal of the tumour (4). As other associated diseases, there was one case each of interstitial pneumonia, depression and parasitic infection of Toxocara canis. In 2 cases, treated with various anti-psychotic drugs for depression and amlodipine for hypertension, the drugs were thought to have triggered the annular erythemas.
DISCUSSION
The most characteristic feature in our case was the extensive annular erythemas with no apparent blister formation. Histopathology showed eosinophilic infiltration in the dermis, but no subepidermal blistering. However, deposition of IgG and C3 along the epidermal basement membrane zone in direct IF and positive results in indirect IF of 1M NaCl-split-skin and BP180 ELISA suggested a diagnosis of BP.
Patient serum was positive in BP180 ELISA, but negative in immunoblot analyses of normal human epidermal extract and BP180 recombinant protein, suggesting a reactivity with conformation-dependent epitope within the BP180 NC16a domain, which was denatured during immunoblot procedure. There is only one previously reported case of this BP variant, in which blister formation was completely absent.
The skin lesions in our case could be treated relatively easily, and did not recur. However, if the skin lesions had continued, it is possible that our case might have developed bullous skin lesions. Hypothetically, autoantibodies to specific antigens or epitopes are responsible in the development of annular erythema, and epitope spreading phenomenon may be involved in changes in clinical features (15). However, our immunological studies did not indicate epitope spreading within BP180 or to other molecules including BP230. Therefore, it is not known, in our case, why the anti-BP180 autoantibodies resulted in erythemas only, but no blisters.

1http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-2254
REFERENCES


