


Tetsuya Ikawa1, Yayoi Tada1*, Takamitsu Ohnishi1, Tomomitsu Miyagaki2, Rei Watanabe2, Norito Ishii3, Takashi Hashimoto4 and Shinichi Watanabe1
Departments of 1Dermatology, Teikyo University School of Medicine, 2-11-1 Kaga, Itabashi-ku, Tokyo 173-8606, 2University of Tokyo Graduate School of Medicine, Tokyo, 3Kurume University School of Medicine, and 4Kurume University Institute of Cutaneous Cell Biology, Kurume, Japan. *E-mail: ytada-tky@umin.ac.jp
Accepted Mar 10, 2016; Epub ahead of print Mar 15, 2016
Bullous pemphigoid (BP) is the most common autoimmune subepidermal bullous disease. BP is mainly caused by immunoglobulin G (IgG) anti-epidermal basement membrane zone (BMZ) antibodies against the NC16a extracellular domain of BP180, and shows marked eosinophilic infiltration (1). Antibodies against intracellular BP230 and the extracellular C-terminal domain of BP180 have also been detected among patients with BP (1).
We report here a rare case of BP, with serum antibodies that reacted only against the 120 kDa LAD-1, which is the ectodomain of BP180, and showed no erythema and eosinophilic infiltration. To date, only 2 cases of BP with IgG antibodies to LAD-1 have been reported (2, 3). We discuss the relationship between the unique clinical and histopathological features and exclusive reactivity with LAD-1 by comparing the current case with similar cases reported previously.
CASE REPORT
A 74-year-old Japanese man visited our clinic with a 6-month history of cutaneous bullae and oral erosions. The patient reported that skin lesions appeared repeatedly on his trunk, extremities, and head, but pruritus and erythema had never been noticed. The patient was being prescribed dipeptidyl peptidase 4 inhibitor for diabetes mellitus, and had a history of hypertension, rheumatoid arthritis, hepatitis C infection and arteriosclerosis obliterans with left iliac artery stent placement, but had no particular family history.
On the first visit, physical examination revealed erosions on the trunk and extremities (Fig. 1a) and a tense bulla on his left foot (Fig. 1b). In addition, erosions were present on the buccal mucosae, soft palate (Fig. 1c) and oropharynx (Fig. 1d). Other mucous membranes were not affected.
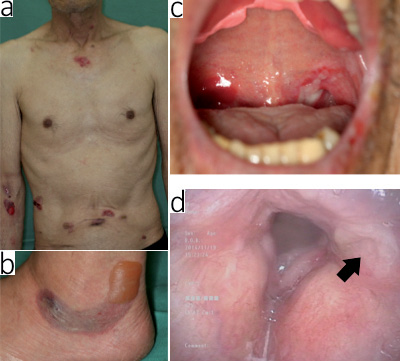
Fig. 1. Clinical features of the patient with bullous pemphigoid. (a) Ruptured blisters on the trunk and arms. (b) A large tense bulla on the left foot. (c) Erosions on the soft palate. (d) Erosion on the oropharynx (arrow).
Laboratory examination revealed an elevated white blood cell count (12,800 µl–1; normal range 3,000–9,800 µl–1) without eosinophilia (1%; normal range 1–8%), and a slightly elevated C-reactive protein level (0.9 mg/dl; normal range 0–0.3 mg/dl). There were elevations of haemoglobin A1c (7.5%; normal range 4.6–6.2%), anti-nuclear antibodies (1:80; normal range 0–1:79), and rheumatoid factor (272 U/ml; normal range 0–14.9 U/ml). Other blood examinations showed normal results. Enzyme-linked immunosorbent assays (ELISAs) did not detect anti-BP180 antibodies or anti-BP230 antibodies.
A skin biopsy specimen obtained from the left hand showed subepidermal separation (Fig. S1a1) with neutrophil infiltration (Fig. S1b1), but minimal infiltration of eosinophils was found. Direct immunofluorescence revealed linear deposits of IgG (Fig. S1c1) and C3 at the BMZ of the lesion, but not IgA. Indirect immunofluorescence using human skin from a normal individual revealed circulating IgG anti-BMZ antibodies at a titre of 1:20, which reacted with the epidermal side of 1M NaCl-split-skin at a titre of 1:20 (Fig. S1d1).
Immunoblotting of normal human epidermal extract revealed that the patient’s IgG antibodies reacted with the full-length BP180 (Fig. S1e1). Immunoblotting using concentrated culture supernatant of HaCaT cells showed that the patient’s IgG, but not IgA, antibodies reacted with the 120 kDa LAD-1 (Fig. S1f1). Immunoblot analysis using recombinant proteins of NC16a and C-terminal domains of BP180, normal dermal extract and purified human laminin-332 did not show any positive reactivity (data not shown).
Based on these findings, the patient was diagnosed with BP due to IgG antibodies against LAD-1. Oral prednisolone at 40 mg/day (8 mg/kg/day) cleared the skin lesions in 2 weeks and the oral lesions in 3 weeks.
DISCUSSION
The case of BP described here is unique with regard to the following points: (i) absence of evident erythema, (ii) absence of pruritus, (iii) mainly neutrophil, but not eosinophil, infiltration into the bullae, and (iv) exclusive reactivity with LAD-1. These unique clinical and histopathological features might be caused by IgG antibodies reacting to a specific epitope on LAD-1.
The IgG antibodies of BP patients generally react with 2 hemidesmosomal components, BP180 and BP230 (4). The BP180 NC16a domain is the immune-dominant region (1, 5), and the sera of 80–90% of patients with BP react against this domain on enzyme-linked immunoassay (ELISA) (1). ELISA of recombinant proteins of both N- and C-terminal domains of BP230 shows positive results in the sera of 60–70% of patients with BP (1). When both BP180 and BP230 ELISA are combined, 90–97% of patients with BP can be diagnosed as having BP (1, 5, 6).
BP180 is the 180 kDa transmembrane glycoprotein of approximately 1,500 amino acids (1) that anchors epithelia to the underlying basement membrane. BP180 consists of a globular intracellular region and an extracellular region, the latter of which is composed of 15 collagenous domains interrupted by 16 non-collagenous domains (4). The NC16a domain exists on the N-terminal region of the extracellular region of BP180. BP sera react less frequently with the BP180 C-terminal domain (1, 4).
LAD-1 was originally found as the target antigen for IgA antibodies in patients with lamina lucida-type linear IgA bullous dermatosis (LABD) (1, 5). LAD-1 is a 120 kDa C-terminal extracellular domain of BP180, and lacks a part of the NC16a domain. LAD-1 was also reported to be targeted by IgG antibodies in BP sera (7). In contrast to LABD, most BP cases with IgG anti-LAD-1 antibodies also reacted with BP230, NC16a and C-terminal domain of BP180 (4, 7). Thus, our patient was unique, because the patient’s sera reacted only with LAD-1. The causative epitope was considered to be located in the 120 kDa domain of BP180, in areas other than those of the recombinant proteins of BP180 NC16a and C-terminal domains.
Our literature survey found 2 other cases of BP with IgG antibodies targeting only LAD-1 (Table SI1). In contrast to our case, these 2 cases did not show mucosal involvement. Interestingly, all 3 cases did not show evident erythema. In addition, one previous case and the present case did not have accompanying pruritus. One previous case and the present case showed neither histopathological eosinophilic infiltration nor blood eosinophilia. Oral prednisolone was effective in one previous case and the present case. Thus, there are common features among these 3 cases.
Various immune responses, including complement activation, inflammatory cell recruitment, release of proteolytic enzymes, and dysfunction of adhesion function lead to blister formation in BP (1, 8). It has been suggested that the IgG antibody titre to the NC16a domain is associated with the clinical severity of BP, whereas the IgG antibody titre to the C-terminal domain is not (9). In addition, IgG reactivity with the C-terminal domain seems to accompany more serious mucosal involvement (1, 9). Thus, reactivity with a different epitope may lead to a distinct immune response. Reactivity with a unique epitope on LAD-1 may have resulted in the unique clinical and histopathological features in the present case.
In conclusion, this patient is the third published case of BP with IgG autoantibodies against only LAD-1, and the first case showing both skin and mucosal symptoms.
ACKNOWLEDGEMENTS
The authors would like to thank Drs A. Fukuyasu, S. Takeoka, K. Hayashi, T. Tanaka, and T. Ishikawa for their helpful advice with the manuscript.
The authors declare no conflicts of interest.

1http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-2400
REFERENCES


