


Nausicaa Malissen1, Jean-Luc Bourrain1, Anca Chiriac2, Aline Montet1, Laure Vincent3, Olivier Dereure1 and Aurélie Du-Thanh1*
1Dermatology Department, 2Pneumology – Allergology Department, Montpellier University Hospital, and 3Clinical Hematology Department, Montpellier University Hospital, 80 avenue Augustin Fliche, FR-34295 Montpellier cedex 5, France. *E-mail: a-du_thanh@chu-montpellier.fr
Accepted Mar 17, 2016; Epub ahead of print Mar 22, 2016
Bortezomib is a selective proteasome inhibitor currently used as standard of care in the treatment of multiple myeloma. Cutaneous side-effects are frequent, as reported in a phase 3 randomized study (1), in which 57% and 70% of patients experienced a grade 3 or higher skin toxicity with subcutaneous and intravenous administration, respectively. However, these adverse effects are usually poorly described in haematological-based reports, and range from benign skin eruption to lethal epidermal necrolysis (2), thus it is important to provide a more specific description when they occur.
CASE REPORT
A 61-year-old man was referred to our department for evaluation of a skin eruption that had developed during the course of chemotherapy implemented for a recently discovered, high-risk smouldering multiple myeloma. He disclosed no other relevant medical background and did not receive any other medication, except for the following regimen, implemented 15 days before occurrence of the skin eruption and combining subcutaneous bortezomib, 1 mg/m2, on days 1, 4, 8 and 11, thalidomide, 100 mg daily, dexamethasone, 40 mg daily from day 1 to day 4, sulfamethoxazole trimethoprim (SMX-TMP) and valaciclovir as prophylactic measures. Initial clinical survey revealed a pruritic and symmetrically distributed intertriginous, maculopapular exanthema, localized to the axillae, antecubital fossae, groin, neck and buttocks (Fig. 1). No clinical symptoms or biological value suggested visceral involvement and/or gravity. Skin biopsy examination displayed only a discrete mixed pericapillary infiltrate. The medical history was not in favour of a contact or irritant reaction. The short delay of occurrence of the skin eruption, the non-erosive intertriginous lesions, the absence of residual pigmentation and the lack of histopathological metaplasia of the eccrine ducts were not in favour of an eccrine squamous syringometaplasia. Thus, the clinical and histopathological pattern rather fulfilled criteria of symmetrical drug-related intertriginous and flexural exanthema (SDRIFE). Cutaneous symptoms rapidly resolved after switching to lenalidomide-dexamethasone regimen. Valaciclovir and SMX-TMP were further re-introduced and well tolerated.
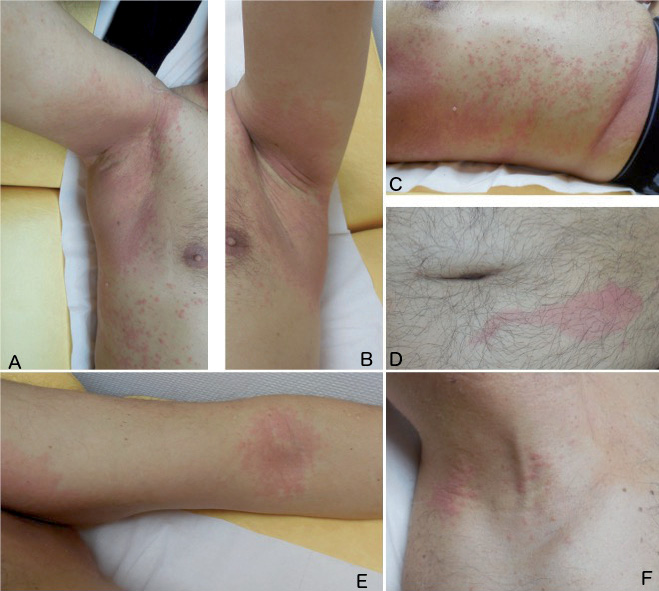
Fig. 1. Symmetrically distributed intertriginous, maculopapular skin eruption localized to (A, B) the axillae, (E) antecubital fossae, (F) neck, with moderate involvement of (C) non-flexural zones, and (D) an erythematous macula at the injection site of bortezomib.
DISCUSSION
SDRIFE (formerly named Baboon syndrome) is a systemic contact dermatitis defined by a number of criteria, as established by Haüsermann et al. (3): (i) exposure to a systemic drug, either upon first systemic administration after a previous primary transcutaneous sensitization (in this case possibly by excessively superficial subcutaneous injections) or upon repeated administration; (ii) sharply demarcated erythema of the gluteal/perianal area and/or V-shaped erythema of the inguinal/perigenital area; (iii) involvement of at least one other intertriginous/flexural localization; (iv) symmetry of the affected area; and (v) absence of systemic symptoms and signs.
A literature search disclosed only one case of SDRIFE due to valaciclovir (4), occurring within 1 h after initial drug intake, which was therefore discordant with our case; on the other hand, bortezomib, thalidomide and SMX-TMP have been much more frequently involved in cutaneous side-effects, but not specifically in SDRIFE occurrence. The context of simultaneous polymedication in this patient made it difficult to establish which drug was individually causative. However, the presence of an erythematous macula at the injection site of bortezomib (Fig. 1) led to this drug being the primary suspect. Three positive (eczematous reaction) intradermal tests using 1:1000, 1:100 and 1:10 dilutions of bortezomib, as shown in Fig. 2, supported this hypothesis. Regarding the availability of injectable bortezomib, we did not proceed to additional patch tests, because when treatment had to be reintroduced rapidly, their eventual negativity would have delayed intradermal tests, which are more sensitive in drug hypersensitivity exploration. Finally, the patient declined further exploration after his treatment was switched. As bortezomib was not re-administered, we cannot conclude with certainty that it is the only causative agent, but strong support resides in the well-tolerated further re-introduction of a drug pharmacologically close to thalidomide (lenalidomide), along with dexamethasone, valaciclovir and SMX-TMP. However, although lenalidomide has some chemical similarity with thalidomide, its tolerance profile is different and its putative role cannot be fully excluded. A final possibility is the simultaneous, although inconspicuous, intake of an analgesic or anti-emetic drug, despite a rigorous medical interrogation and a close follow-up in this context of polymedication.

Fig. 2. Positive intradermal tests on the forearm using 1:1000, 1:100 and 1:10 dilutions of bortezomib.
A variety of skin reactions have been reported with bortezomib, either with the intravenous form (Sweet’s syndrome (5), cutaneous lupus (6, 7), perivasculitis lymphocytic infiltrate with atypical CD30 (8)) or with the subcutaneous form (necrotic local reaction at the injection sites (9)) of this drug.
Although re-introduction could not be performed, this case of SDRIFE related to bortezomib further emphasizes the importance of dermatological expertise in identifying more specific subsets of so-called “rashes” in therapeutic trials, especially in malignancies in which a number of pathomechanisms may be discussed, if not associated.
The authors declare no conflicts of interest.
REFERENCES

