


Elaha Salik1, Ida Løvik1, Klaus E. Andersen1,2 and Anette Bygum1
1Department of Dermatology and Allergy Centre, Odense University Hospital, and 2Centre for Innovative Medical Technology, Institute of Clinical Research, University of Southern Denmark, Odense, Denmark
There is increasing awareness of reactions to vaccination that include persistent skin reactions. We present here a retrospective investigation of long-lasting skin reactions and aluminium hypersensitivity in children, based on medical records and questionnaires sent to the parents. In the 10-year period 2003 to 2013 we identified 47 children with persistent skin reactions caused by childhood vaccinations. Most patients had a typical presentation of persisting pruritic subcutaneous nodules. Five children had a complex diagnostic process involving paediatricians, orthopaedics and plastic surgeons. Two patients had skin biopsies performed from their skin lesions, and 2 patients had the nodules surgically removed. Forty-two children had a patch-test performed with 2% aluminium chloride hexahydrate in petrolatum and 39 of them (92%) had a positive reaction. The persistent skin reactions were treated with potent topical corticosteroids and disappeared slowly. Although we advised families to continue vaccination of their children, one-third of parents omitted or postponed further vaccinations. Key words: persistent skin reactions; aluminium hypersensitivity; pruritic nodule; contact allergy; childhood vaccinations.
Accepted Apr 6, 2016; Epub ahead of print Apr 12, 2016
Acta Derm Venereol 2016; 96: XX–XX.
Anette Bygum, Department of Dermatology and Allergy Centre, Odense University Hospital, DK-5000 Odense C, Denmark. E-mail: anette.bygum@rsyd.dk
Aluminium is a ubiquitous metal, which is used for many different purposes, e.g. in cooking utensils, building materials, consumer products, antiperspirants and other cosmetics (1). Aluminium is used as an adjuvant in vaccines and allergen immunotherapy, to enhance a specific and longer-lasting immune response, although the exact mechanism remains a target of research (2). Persistent pruritic and infiltrated skin reactions after vaccinations have been reported in the literature since the 1960s (3–6). Later studies have shown an association between persistent skin reactions after vaccinations and contact allergy to aluminium (7–9). Originally, these adverse effects have been considered rare and were primarily described in case studies. However, in 2003, a Swedish study showed a 0.8% incidence of persistent pruritic nodules (645 cases of 76,000 vaccinated children) related to aluminium-adsorbed childhood vaccines produced by Statens Serum Institut (SSI) in Denmark, and contact allergy to aluminium was demonstrated in 77% of the tested patients (10). This is consistent with a recent Swedish prospective cohort study reporting an incidence of 0.83% of “itching vaccination granulomas” (7). Several of the vaccines available in Denmark are adsorbed to aluminium, including vaccines in the Danish vaccination programme for children (Table SI1). The incidence of persistent skin reactions after vaccination in Denmark is unknown.
The aim of this retrospective study of patients with persistent skin reactions after vaccination in Denmark was to investigate the occurrence, clinical presentation, diagnostic work-up, course and consequences with regard to future vaccinations.
METHODS
Ethics
Permission to process personal data was obtained from the Danish Data Protection Agency (jr. no. 2014-41-2979). Permission from an ethics committee was not needed for this observational study.
Participants/questionnaires
Patients were identified through the department’s diagnosis code system (T88.1B vaccination granuloma) and a contact allergy database (The Allergen Bank), collecting patch-test data from approximately 70 dermatologists in private practice and 4 dermatology departments in Denmark. The patients included in the study were tested for delayed hypersensitivity to aluminium, by patch-testing with 2% aluminium chloride hexahydrate in petrolatum from January 2003 to October 2013.
To differentiate reactions caused by aluminium in childhood vaccines and those caused by other sources of aluminium, only children aged 10 years or younger at the time of testing were included. A total of 118 patients were tested for aluminium hypersensitivity during the 10-year period; 73 patients older than 10 years (median age 45 years) were excluded (Fig. 1). Data were collected from the medical records, and questionnaires were sent to the parents of the children in order to collect data on clinical manifestations, duration, treatment, consequences on the childhood vaccination programme and reporting of the adverse effect.
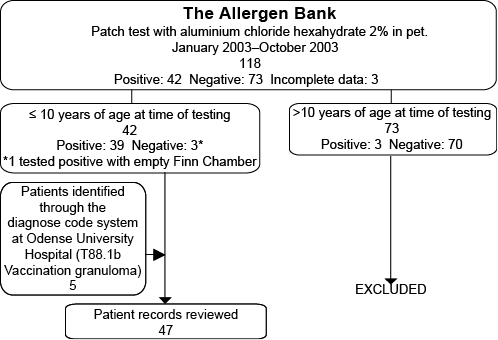
Fig. 1. Included and excluded patients.
RESULTS
A total of 47 children with persistent skin reactions after vaccination were identified, comprising 23 girls and 24 boys with a mean age of 32 months (age range 3 months–6.3 years). The majority of children had been tested during the last 2 years. Thirty-nine of 42 children who were patch-tested had positive reactions to 2% aluminium chloride hexahydrate in petrolatum. One patient with a negative test had a positive reaction to an empty Finn Chamber and was also considered positive, giving a total of 40 children with positive tests. Five children were diagnosed clinically based on a typical history and presentation. In 74% of the children (28 of 38 for whom data was available), the reaction was most likely related to the third dose of the diphtheria, tetanus, acellular pertussis, inactivated polio vaccine/Haemophilus influenzae b conjugate (DTaP-IPV/ Hib) vaccine given at 12 months of age (Table I).
Table I. Clinical data regarding vaccination granulomas and aluminium hypersensitivity after childhood vaccination collected from 47 medical records and 39 returned parental questionnairesa
|
Suspected vaccine associated with the itching nodules and aluminium hypersensitivity |
|
|
1st dose DTaP-IPV/Hib + PCV |
3/38b |
|
2nd dose DTaP-IPV/Hib + PCV |
5/38 |
|
3rd dose DTaP-IPV/Hib + PCV |
21/38 |
|
3rd dose DTaP-IPV/Hib + PCV/1st dose measles, mumps rubella |
7/38 |
|
DTaP-IPV Booster |
1/38 |
|
Bacillus Calmette-Guérin |
1/38 |
|
Most common manifestations |
|
|
Itching |
45/47 |
|
Nodules/granulomas |
32/47 |
|
Excoriations |
17/47 |
|
Eczema |
16/47 |
|
Hyperpigmentation |
15/47 |
|
Hypertrichosis |
11/47 |
|
Infiltration |
9/47 |
|
Induration |
7/47 |
|
Superficial wounds |
6/47 |
|
Intensity of symptoms |
|
|
Mild (minor symptoms) |
3/42 |
|
Moderate (episodic itching and irritation) |
30/42 |
|
Severe (intense itching and sometimes interruption of sleep) |
9/42 |
|
Duration of symptoms at time of testing |
|
|
0–6 months |
10/43 |
|
> 6–12 months |
20/43 |
|
> 12–18 months |
6/43 |
|
> 18–24 months |
4/43 |
|
> 2 years |
3/43 |
|
Treatment |
|
|
Topical corticosteroids |
36/47 |
|
Topical corticosteroids under occlusion |
17/47 |
|
Occlusion only |
1/47 |
|
Antihistamines |
2/47 |
|
Antipruritic cream |
3/47 |
|
Tacrolimus/pimecrolimus |
2/47 |
|
Antibiotics |
1/47 |
|
Excision |
2/47 |
|
Homeopathic treatment |
1/47 |
|
No treatment |
7/47 |
|
Efficacy of treatment |
|
|
Modest effect |
9/29 |
|
Partial effect |
12/29 |
|
Full effect |
2/29 |
|
No effect |
6/29 |
aDenominator represents number of answers. bOne patient had reactions after both 1st and 3rd doses.
DTaP-IPV/Hib: diphteria, tetanus, acellular pertussis, inactivated polio vaccine/Haemophilus influenzae b conjugate; PCV: pneumococcal conjugate vaccine.
All but 2 patients had itching as their main symptom, and two-thirds had a deep nodular infiltrate, also referred to as a granuloma (Table I and Fig. 2). Seventy-one percent of the children had moderate discomfort with episodic itching, and 21% of the children had severe symptoms with intense itching, sometimes causing interrupted sleep. The majority of children were treated with topical corticosteroids, sometimes under occlusion. The efficacy of this treatment was described by the parents as moderate.
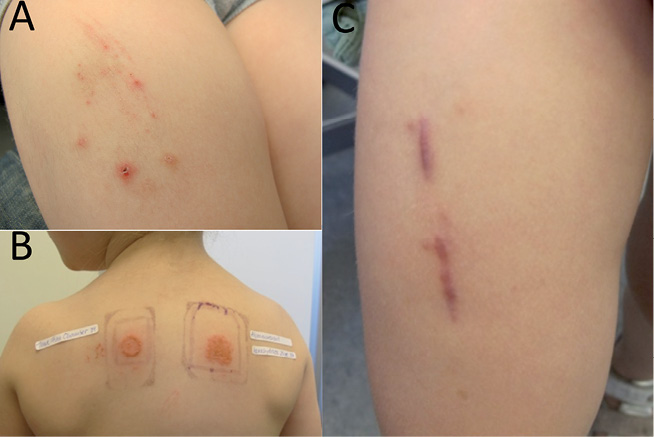
Fig. 2. Clinical signs of persistent skin reactions and aluminium hypersensitivity. (A) Excoriations, hyperpigmentation, hypertrichosis and eczema on the lateral thigh. (B) Patch-test showing positive reaction (+++) on the 4th day to an empty Finn Chamber (left) and to aluminium chloride hexahydrate 2% (right). C. Two scars on the left thigh of a 3-year-old child after surgical removal of 3 itching nodules.
Three children experienced aggravation of symptoms during systemic infections, and 4 reacted anamnestically to aluminium-containing products (raisins, bread mix, sunscreens and aluminium containers), although these reactions were not further specified.
At the time of the query, 66% of the children had received all the planned vaccinations, whilst 34% of the parents had chosen to postpone or omit further vaccination of their child.
The families received the questionnaires at a median of 1.6 years (range 6 months to 9.5 years) after contact with a dermatologist. Eighty-four percent of the children (32 of 38 for whom data was available) had ongoing symptoms at the time of query, despite the fact that 74% (28 of 38 for whom data was available) had been treated with potent topical corticosteroids. Five children had been through a complex diagnostic process involving departments of paediatrics, orthopaedic and plastic surgery, including different radiological imaging techniques and histopathological examinations of skin specimens, before the condition was recognized. In 2 patients malignancy was suspected, and one child had the nodule surgically removed under general anaesthesia (Fig. 2C). In another, the nodule was removed due to the parents’ concern and lack of a precise diagnosis. Two patients had skin biopsies from their skin lesions and 2 patients had the nodules surgically removed. One skin biopsy showed fibrosis and the other 3 biopsies showed chronic inflammation.
Twenty-eight of these adverse reactions to childhood vaccines (60%) were reported to the Danish Health and Medicines Authority (DHMA) by physicians or parents, and 7 of these reactions were also reported to the Danish Patient Compensation Association (PCA).
DISCUSSION
The majority of children were seen and tested in 2012 and 2013, illustrating an apparent increase in the number of children referred with persistent skin reactions and aluminium hypersensitivity in the last decade. In everyday language, we refer to and encode these skin reactions as vaccination granulomas, although this is in fact a misnomer, as granuloma should be a histopathological description. There is also an increased number of reported cases to DHMA and PCA (personal correspondence by Peter Jakobsen, the Danish Patient Compensation Association and Mai Frederiksen Raun, the Danish Health and Medicines Authority). This is likely to be a result of an increased awareness among healthcare professionals and the general public, rather than an actual increase in incidence. In Denmark aluminium hydroxide is the most frequently used adjuvant, and vaccines without aluminium are not available at present. SSI previously produced a diphtheria-tetanus (DT)-vaccine without aluminium (11, 12), but it was withdrawn from the market due to the lack of randomized controlled studies confirming efficacy and safety. As vaccines are given to healthy children on a large scale, the acceptable rate of adverse effects is relatively lower than that for other pharmaceuticals. Although the overall rate of adverse effects to vaccines is low (13), there is a growing scepticism among the general public regarding vaccine safety.
It has been suggested that the risk of persistent skin reactions at the injection sites are higher following subcutaneous injections compared with intramuscular injections (14), although the importance of the injection technique may be overrated (7). Intramuscular injection has been the standard recommendation for aluminium-containing vaccines in Denmark since 1999 (15). We know, however, that the administration of vaccines to children can be challenging, and even with an intramuscular injection, it can be difficult to avoid depositing some of the vaccine content subcutaneously.
Forty-seven cases of suspected “vaccination granulomas” and aluminium allergy were reported to the DHMA in 2013 (Fig. 3). Supposing that the incidence of 0.83% is applicable for the Danish population vaccinated with the aluminium-adsorbed childhood vaccines produced by SSI, there would be approximately 450 cases of “vaccination granulomas” or persistent skin reactions every year (0.83% × 55,873 (the Danish birth cohort in 2013)). We know that not all side-effects are reported by physicians or patients, but assume that these reactions may also be overlooked by the families of the children and healthcare personnel. Five patients from our own department were diagnosed with persistent skin reactions after vaccination, based on clinical features. This may also be the case in private practices, where diagnosis codes are not used. Four children were primarily referred to departments of paediatrics and, for 2 of these patients, the nodular skin lesions were removed surgically.
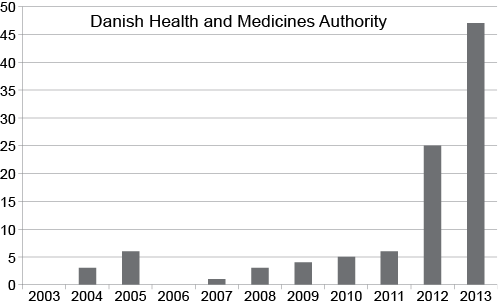
Fig. 3. Number of passively reported cases of persistent skin reactions and/or persistent skin reactions and aluminium allergy.
Clinical features and time course
The most prevalent symptom in this study was long-lasting, pruritic nodules at the injection sites, and this has been similarly documented previously (6, 7, 16–19). Excoriations, eczema, hyperpigmentation, hypertrichosis and infiltration were other frequently observed symptoms. According to the literature, the symptoms vary over time, with a more intense primary phase and a less eventful healing phase (18). Lidholm et al. and Bergfors & Trollfors described a flare of symptoms during intercurrent infections (7, 18), as was the case for 3 patients in the current study.
For the majority of patients, the symptoms occurred after the third dose of DTaP-IPV/Hib. A similar observation was made in 3 other studies (7, 10, 18). This suggests a correlation between the number of injections with aluminium-adsorbed vaccines and the onset of symptoms. Only one of our patients had a reaction to the DTaP-IPV booster vaccine administered at the age of 5 years, which is also in accordance with results from other studies (10, 16, 18). Young age seems, therefore, to be a risk factor for developing persistent skin reactions and aluminium hypersensitivity (20, 21). Another possible explanation could be the accumulated aluminium load in the 1-year-old child, for whom up to 6 aluminium-adsorbed vaccines are administered during the first year of life. Typically, there is a lag phase between vaccination and manifestation of symptoms that may complicate the diagnostic process. Based on the duration of symptoms and the assumed triggering vaccine, as reported by the parents in this investigation, there was a great variation in the latency period, ranging from 0 to 18 months. Lidholm et al. (7) reported a median latency of 2.5 months (range 2 weeks to 13 months).
Contact allergy and allergic contact dermatitis to aluminium
A total of 93% (39/42) of our tested patients had positive patch tests to 2% aluminium chloride hexahydrate in petrolatum, and one patient reacted to an empty Finn Chamber. Bergfors and colleagues reported a prevalence of positive patch-test reactions of 77–95% among children with persistent skin reactions (7, 10, 18).
Treatment response, prognosis and consequences
The treatment of pruritic vaccination granulomas is symptomatic, with the intention being to break the itch-scratch cycle. Most of the children in our study were treated with topical steroids of potency groups I–IV, and sometimes also with occlusion. The efficacy of the treatment was often judged by the parents to be unsatisfactory, and a total of 32 of 38 patients in this study had ongoing nuisance, lasting a median of 1.6 years (range 6 months to 9.5 years) at the time of this study.
The parents described allergic reactions to aluminium-containing products in 4 children; however, these reactions were not further specified or confirmed. Bergfors & Trollfors (18) reported 11 cases of allergic contact dermatitis reported by the parents following contact with aluminium containing deodorants, cosmetics, sunscreens and buttons, but the reactions were not objectively confirmed.
The long-term prognosis of aluminium hypersensitivity has been investigated in a few studies. Kaaber et al. (19) retested 4 patients previously diagnosed with aluminium hypersensitivity and vaccination granulomas. Two of them no longer had positive patch-tests and they had no symptoms related to the formerly pruritic nodules. Lidholm et al. (17) retested 241 children with long-lasting itchy subcutaneous nodules previously diagnosed with aluminium allergy. After a follow-up of 5 years or longer, 186 patients had negative patch-tests. A negative patch-test correlated significantly with the disappearance of clinical symptoms, increasing age, time elapsed since first vaccination and test severity of the first positive patch-test. Only 3 of 73 tested patients >10 years of age, registered in the Allergen bank, had positive patch tests. This supports the hypothesis that aluminium allergy in relation to childhood vaccinations is temporary and is not necessarily maintained in adulthood. The questionnaires in the current study revealed that one-third of the parents had decided to omit or postpone further vaccination of their child. However, only one of the re-vaccinated children developed renewed symptoms in the current study. Another study showed that only 2 out of 25 re-vaccinated children developed new pruritic skin lesions, which were less severe than earlier reactions (17). Based on these observations, it seems safe to be re-vaccinated with aluminium-adsorbed vaccines despite previous vaccination granuloma and aluminium allergy.
Study limitations
The results of this study are based on retrospective data from medical records and questionnaires sent to the parents of a selected group of children and may, therefore, have limitations due to recall bias and selection of patients. The patient records were inadequate with regard to some of the questions, e.g. vaccination history and status as well as specified reactions to aluminium-containing products. There may also be some variation in the interpretation of information from the medical records. Follow-up data are limited, as most patients were followed for a short period of time, although data from questionnaires to the parents gave some further information on the course.
Conclusion
Awareness of vaccination reactions and persistent skin reactions is increasing, and the condition seems to be more common than previously assumed; however, it may still be overlooked. Persistent skin reactions and aluminium hypersensitivity are closely related and can be a long-lasting nuisance. We advise treatment with potent topical corticosteroids to break the itch-scratch cycle. The condition may cause unnecessary anxiety for the children and their families, who may postpone or opt out of further vaccination. This was the case for approximately one-third of the patients in the current study. Healthcare personnel, including paediatricians and surgeons, should recognize this very characteristic condition with long-lasting pruritic nodular infiltrates at former injection sites of aluminium-containing vaccines in order to avoid unnecessary imaging or surgery. We find it valuable to patch-test these children to support the significance of aluminium allergy. Parents should be encouraged to allow their children to follow the vaccination programme as scheduled, and physicians should administer aluminium-containing vaccines intramuscularly.
ACKNOWLEDGEMENTS
The authors would like to thank the parents who answered questionnaires about their children and all the dermatologists who provided information from the medical records of patients tested for aluminium contact allergy. Gitte Strauss, Mads Nielsen and Anne Danielsen, Hudklinikken Panoptikon – København, Allergilaboratoriet, Hudklinikken Aarhus Universitetshospital, Lars Halkier-Sørensen and Sanne Krogsbøll Buus, Hudklinikken – Horsens, Christin Maier, Hudklinikken – Silkeborg, Tove Agner, Dermatologisk afdeling, Bispebjerg Hospital, Gregor Jemec, Dermatologisk afdeling, Roskilde Sygehus, Ida-Marie Stender, Hudklinikken på Jægersborg Allé – Charlottenlund, Jens Sindrup, Hudklinikken Amagerbrogade – København, Marianne Kollander, Hudklinikken – Randers, Søren Frankild, Hud og laserklinikken – Esbjerg, Michaela Bruhns, Hudklinikken – Næstved, Sanne Pedersen Fast, Hudklinikken – Fredericia, Wioletta Kubicka, Hudklinikken – Vordingborg.
The authors declare no conflicts of interest.

1http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-2432
REFERENCES


