


Minna E. Kubin1, Päivi M. Hägg1, Nina Kokkonen1, Kirsi-Maria Haapasaari2, Juha P. Väyrynen2, Tatsuya Uchida3, Virpi Glumoff3, Petri Kulmala3,4, Tiina Hurskainen1 and Kaisa Tasanen1
1PEDEGO Research Unit, Oulu Center for Cell-Matrix Research, Department of Dermatology and Medical Research Center Oulu, Oulu University Hospital and University of Oulu, 2Department of Pathology and Medical Research Center Oulu, Oulu University Hospital and University of Oulu, 3Research Unit of Biomedicine, Medical Microbiology and Immunology, University of Oulu, and 4PEDEGO Research Unit, Department of Children and Adolescents and Medical Research Center Oulu, Oulu University Hospital and University of Oulu, Oulu, Finland
First-line treatments of bullous pemphigoid (BP) are topical and systemic glucocorticoids (GC). The actions of GCs are mediated by glucocorticoid receptors (GR), which exist in several isoforms, of which GRα and GRβ are the most important. In many inflammatory diseases, up-regulation of GRβ is associated with GC insensitivity. The aims of this study were to determine the expression of GRα and GRβ in patients with BP and to investigate the effect of prednisolone treatment on the expression of GR isoforms in BP. Quantitative real-time PCR (qPCR) analysis demonstrated that GR isoform mRNAs are expressed in peripheral blood mononuclear cells (PBMC) from patients with BP. Expression of GRα and GRβ protein was confirmed by immunohistochemical staining of BP skin biopsies and by Western blot analysis and flow cytometric analysis of PBMCs. During prednisolone treatment, GRα and GRβ expression varied markedly, but changes were not suitable as a clinical marker of GC sensitivity in patients with BP. Key words: bullous pemphigoid; glucocorticoid receptor alpha; glucocorticoid receptor beta.
Accepted Apr 14, 2016; Epub ahead of print Apr 19, 2016
Acta Derm Venereol 2016; 96: XX–XX.
Minna Kubin, Department of Dermatology, Oulu University Hospital, Kajaanintie 50, FIN-90029 Oulu, Finland. E-mail: minna.kubin@ppshp.fi
Bullous pemphigoid (BP) is by far the most common autoimmune blistering disease, typically affecting the skin and mucous membranes in elderly patients (1–3). BP presents with severe itch, localized or generalized blisters and erosions. Systemic and topical glucocorticosteroids (GC) are the best-evaluated treatment for BP, while evidence of the effectiveness of adjuvant, corticosteroid-sparing therapy is poor (1–3). Patients with BP have increased risk of death; their poor prognosis is due to old age, associated medical conditions and the side-effects of high-dose systemic corticosteroids used for treatment of severe BP (1–3).
The actions of GCs are mediated by intracellular glucocorticoid receptors (GR) (4). By alternative splicing, different GR isoforms, GRα, GRβ, GRγ, GR-A and GR-P, are generated (4, 5). Clinically, GRα and GRβ are the most important. In many inflammatory diseases, such as asthma (6), ulcerative colitis (7), rheumatoid arthritis (8) and systemic lupus erythematosus (9), up-regulation of GRβ has been shown to be associated with GC insensitivity (10). Although the long-term use of systemic and topical corticosteroids is the first-line treatment of BP, to our best knowledge, the work by Liu et al. (11) is the only study looking at the effect of corticosteroid treatment on the expression of GR isoforms in the skin of patients with BP.
The aims of this study were to evaluate the expression of GRα and GRβ in patients with BP and to conduct a prospective follow-up study to measure whether the expression of GR isoforms is altered during treatment of BP with systemic corticosteroids.
MATERIALS AND METHODS
The ethics committee of the Northern Ostrobothnia Hospital District approved the study, which was performed according to the principles of the Declaration of Helsinki 2013. Written consent for scientific purposes was obtained from all participants.
Patients and blood samples
The study population comprised 16 patients with BP and 17 elderly control patients with non-melanoma skin cancer. Inclusion criteria for patients with BP were: recently started severe symptoms (generalized itch, widespread blistering); not receiving any systemic treatment for BP; and not receiving systemic GC therapy for any other disease before entering the study. The symptoms of patients with BP had started within 1–10 weeks before admittance to our clinic. The diagnosis of BP was based on typical clinical presentation, direct immunofluorescence microscopy and serology (1). Circulating autoantibodies against recombinant human BP180 protein’s NC16A domain were measured at HUSLAB (Helsinki, Finland) using the BP180 enzyme-linked immunoassay (ELISA) kit (MBL, Medical & Biological laboratories Co., Ltd, Nagoya, Japan). Systemic GC therapy with prednisolone (Prednisolone®, Leiras, Helsinki, Finland) and topical treatment with medium or potent corticosteroid was started on all patients with BP. Peripheral blood samples were taken before onset of prednisolone treatment and on days 5, 14 and 60 during treatment. Peripheral blood mononuclear cells (PBMC) were isolated from heparinized blood samples (20 ml) using the Ficoll-Paque Plus® density-gradient method (GE Healthcare Biosciences, Uppsala, Sweden). A lesional skin biopsy was taken from the upper arm or truncal skin from 11 patients with BP prior to treatment.
Quantitative real-time PCR (qPCR)
Total mRNA was isolated from PBMCs with the Oligotex Direct mRNA Mini Kit (Qiagen, Crawley, UK) and reverse transcribed using M-MuLV reverse transcriptase (Fermentas, Helsinki, Finland). Quantitative real-time PCR (qPCR) was performed with IQ5 Real-Time PCR Detection System and iQ™ SYBR® Green Supermix (both from Bio-Rad, Hercules, CA, USA) to quantify GRα (GenBank access number X03225) and GRβ (X03348.1) transcripts. The transcripts of human glyceraldehyde-3-phosphate dehydrogenase (GAPDH, NM_002046) and of human β-actin (NM_001101.3) served as controls. The primers used are shown in Table I.
Table I. Primers used for qPCR
|
Primer |
|
|
Common upstream primer for hGRα and hGRβ |
5’-CCTAAGGACGGTCTGAAGAGC-3’ |
|
hGRα downstream primer |
5’-GCCAAGTCTTGGCCCTCTAT-3’ |
|
hGRβ downstream primer |
5’-CCACGTATCCTAAAAGGGCAC-3’ |
|
GAPDH upstream primer |
5’-GGAGCCAAAAGGGTCATCATC-3’ |
|
GAPDH downstream primer |
5’-GTCATGAGTCCTTCCACGATA-3’ |
|
β-actin upstream primer |
5’-AGAGCTACGAGCTGCCTGAC-3’ |
|
β-actin downstream primer |
5’-AGCACTGTGTTGGCGTACAG-3’ |
hGR: human glucocorticoid receptor; GAPDH: glyceraldehyde-3-phosphate dehydrogenase.
Melt curve analysis was performed to ensure the amplification of a single product. Expression levels were estimated by the normalized expression method (∆∆Ct) according to the manufacturer’s instructions (BioRad).
Western blot analysis
Western blot analyses from PBMCs of 6 patients with BP and 5 controls were performed as described previously (12). Briefly, a novel GRβ-specific antibody (Eurogentec, Seraing, Belgium) and antibody detecting both GRα and GRβ isoforms (Santa Cruz Biotechnology, Inc., Santa Cruz, CA, USA) were used; GAPDH (Santa Cruz Biotechnology, Inc.) served as a loading control. HaCaT (spontaneously transformed immortal keratinocyte cell line from adult human skin) cells served as a positive control sample.
Immunohistochemical analysis of skin biopsies
Immunohistochemical staining of lesional skin biopsies was performed using Invitrogen Histostain®-Plus Bulk kit (Invitrogen, Camarillo, CA, USA). Primary antibodies for GRα (sc-1002 (p-20); Santa Cruz Biotechnology Inc.) and for GRβ (ab3581; Abcam, Cambridge, UK) were used at dilutions of 1:500 and 1:1000, respectively.
Flow cytometric analysis (FCM)
PBMC samples were immunophenotyped using a 4-colour flow cytometry panel with FACSCalibur (Becton Dickinson, Mountain View, CA, USA) cytometer and analysed with FlowJo software version 7.6.5 (Treestar, Ashland, USA). 0.5×105 PBMCs were fixed in 4% paraformaldehyde and permeabilized with 0.5% saponin. The cells were first stained in PBS, 0.5% bovine serum albumin (BSA), 0.5% saponin-buffer with anti-GRβ rabbit polyclonal Ab (Eurogentec) followed by PE-conjugated anti-rabbit Ig goat polyclonal secondary Ab (ab97070, Abcam). Subsequently, anti-CD3 PerCP (BD 345766), anti-CD4 APC (BD 555349) and anti-GR mouse monoclonal FITC detecting GRα and GRβ isoforms (G3030-01M, USBiological, Salem, MA, USA) were used for antigen staining of the cells. A total of 10,000 cells were acquired for the analysis. Corresponding isotype control antibodies were used as negative controls in all assays.
Expression of GRα+β and GRβ proteins was analysed in CD4+/CD3+; CD4–/CD3+; CD4low/CD3– and CD4–/CD3– cells.
Statistical analysis
Statistical analyses were conducted using IBM SPSS Statistics 22.0 (IBM, Chicago, IL, USA). Spearman’s ρ was used to evaluate statistical difference between the dosage of prednisolone and GR isoform mRNA levels, as well as BP180 level and GR isoform pretreatment levels. Wilcoxon signed-ranks test was used to compare the expression of GR isoform mRNA levels before and during prednisolone treatment.
RESULTS
Clinical characteristics and treatment of patients with bullous pemphigoid
BP diagnosis was confirmed by positive direct immunofluorescence staining, positive serology and typical clinical features. Prednisolone treatment was initially started at a dosage of 0.38–0.69 mg/kg/day (mean 0.49 mg/kg/day). In the majority of patients with BP, the prednisolone dosage was gradually diminished, since the response to treatment was considered good according to the clinical condition. Three of the patients (BP1, BP2 and BP13) experienced aggravation of the disease, and azathioprine was thus initiated as an adjuvant therapy (Table II).
Table II. Clinical characteristics of patients with bullous pemphigoid (BP) and expression of glucocorticoid receptors GRα and GRβ compared with the pretreatment level (marked as 1-fold) during systemic corticosteroid treatment in peripheral blood mononuclear cells (PBMCs) analysed by quantitative real-time PCR (qPCR)
|
|
Sex/age, years |
BP180 ELISA |
Initial dosage of prednisolone |
Adjuvant therapy |
Topical corticosteroid |
Pretreatment |
GRα |
|
|
GRβ |
||||
|
5 days |
14 days |
60 days |
Pretreatment |
5 days |
14 days |
60 days |
||||||||
|
BP1 |
M/71 |
136 |
0.61 |
Azathioprine |
Bm |
1.00 |
0.66 |
0.78 |
0.05 |
|
1.00 |
ND |
2.15 |
ND |
|
BP2 |
F/80 |
132 |
NA |
Azathioprine |
Bm |
1.00 |
0.63 |
3.20 |
2.95 |
|
1.00 |
1.05 |
1.87 |
0.63 |
|
BP3 |
M/87 |
73 |
0.44 |
|
Bm |
1.00 |
0.68 |
3.09 |
1.39 |
|
ND |
ND |
10.68 |
2.49 |
|
BP4 |
F/89 |
116 |
0.5 |
|
Hcb |
1.00 |
0.69 |
0.70 |
0.57 |
|
1.00 |
2.05 |
5.34 |
7.63 |
|
BP5 |
F/75 |
6a |
0.48 |
|
Bm |
1.00 |
2.25 |
0.64 |
2.74 |
|
1.00 |
0.60 |
0.64 |
0.44 |
|
BP6 |
F/88 |
128 |
0.69 |
|
Bm |
1.00 |
1.01 |
0.81 |
0.75 |
|
1.00 |
10.75 |
ND |
1.44 |
|
BP7 |
M/66 |
108 |
0.44 |
|
Bm |
1.00 |
1.24 |
0.77 |
2.04 |
|
1.00 |
0.92 |
ND |
0.96 |
|
BP8 |
M/81 |
90 |
0.44 |
|
Bm |
1.00 |
NA |
NA |
1.38 |
|
1.00 |
NA |
NA |
0.47 |
|
BP9 |
F/83 |
20 |
0.45 |
|
Bm |
1.00 |
2.23 |
1.25 |
1.97 |
|
1.00 |
1.12 |
0.70 |
ND |
|
BP10 |
F/75 |
179 |
0.41 |
|
Bm |
1.00 |
1.42 |
1.64 |
1.28 |
|
1.00 |
2.44 |
ND |
ND |
|
BP11 |
M/75 |
41 |
0.38 |
|
Bm |
1.00 |
1.24 |
NA |
1.30 |
|
ND |
2.44 |
NA |
0.58 |
|
BP12 |
F/71 |
100 |
0.48 |
|
Hcb |
1.00 |
NA |
2.21 |
1.53 |
|
1.00 |
NA |
0.64 |
0.43 |
|
BP13 |
M/74 |
140 |
0.54 |
Azathioprine |
Bm |
1.00 |
0.87 |
1.02 |
0.63 |
|
1.00 |
1.96 |
6.81 |
1.28 |
|
BP14 |
F/79 |
55 |
0.49 |
|
Bm |
1.00 |
5.07 |
1.80 |
NA |
|
1.00 |
1.71 |
ND |
NA |
|
BP15 |
M/85 |
< 5a |
0.44 |
|
Bm |
1.00 |
0.57 |
NA |
1.03 |
|
ND |
1.10 |
NA |
1.78 |
|
BP16 |
F/89 |
17 |
0.62 |
|
Bm |
1.00 |
1.11 |
NA |
NA |
|
1.00 |
3.51 |
NA |
NA |
aEven though the BP180 ELISA was negative (< 9 U/ml) in 2 patients (BP5 and BP15) they were considered to have BP based on the typical clinical picture and positive direct immunofluorescence.
Bm: betamethasone, Hcb: hydrocortisone butyrate, NA: not analysed, ND: not detected.
Expression of GRα and GRβ in bullous pemphigoid
Baseline expression levels of GR isoform mRNAs in PBMCs isolated from BP patients and controls were quantified using qPCR. GRα was present in all 16 BP and 17 control samples, whereas the expression of GRβ was detected in 13 of the BP samples and 12 of the control samples (Fig. 1a). Mean values of both isoform mRNA levels were higher in control patients, but the difference was not statistically significant (Fig. 1a). GR isoform levels did not correlate with the BP180-ELISA values.
Immunoblotting of PBMC lysates with an antibody detecting both GRα and GRβ showed the presence of a 94-kDa band in all the BP samples analysed and nearly all control samples, confirming the expression of GRα (Fig. 1b). Immunoblotting with a GRβ-specific antibody detected the 90-kDa GRβ band in 4 out of 6 patients and in all control samples with variable intensity (Fig. 1b). GRα+β and GRβ proteins were also detected in all the PBMC samples studied by FCM. Staining with GRα+β was similar in both CD4+ T cells and CD4– T cells. CD4+ non-T cells stained more with GRβ than T cells. The results did not differ between BP patients and controls (Fig. 1c).
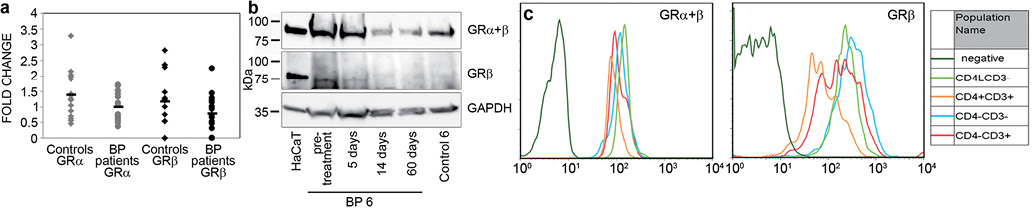
Fig. 1. Expression of glucocorticoid receptor (GR) isoforms in bullous pemphigoid (BP) patients’ peripheral blood mononuclear cell (PBMC) samples. (a) Pretreatment expression of GR isoform mRNAs in PBMCs analysed by quantitative real-time PCR (qPCR). GRα mRNA expression was higher in control patients (mean ± standard deviation (SD) 1.39 ± 0.77, range 0.47–3.30) than in patients with BP (mean ± SD 1.01 ± 0.93; 0.37–1.70). A similar difference was found with GRβ expression: the mean ± SD was 1.19 ± 0.46 (0.00–2.82) and 0.8 ± 0.60 (0.00–2.25) in controls and patients with BP, respectively. Expression levels were compared with the expression in HaCaT cells. Mean values are marked with bars. (b) Expression of GR proteins. A representative Western blot analysis of GR protein expression in PBMCs. A 94-kDa GRα-specific band was detected in cultured HaCaT cells (serving as a positive control) and in PBMCs collected at different time points from patient BP 6 and Control 6. A 90-kDa GRβ-specific band was detected in cultured HaCaT cells as well as in patient samples prior to GC treatment and on day 5. On days 14 and 60 only a faint protein band was detected in correlation with the decreasing mRNA levels measured by qPCR. In the PBMC sample from Control 6, only a faint 90-kDa band was detected. GAPDH (37-kDa) served as a loading control. (c) Flow cytometry of PBMC. Frozen cells were stained with CD3-, CD4-, GRα+β- and GRβ-specific antibodies. Representative stainings of GRα+β and GRβ proteins are shown. GRα+β is expressed equally in leukocytes, whereas GRβ expression varies among different cell populations.
Immunohistochemical staining of lesional BP skin biopsies demonstrated only a weak cytoplasmic staining with the GRα antibody in keratinocytes, whereas the GRβ immunostaining was strong and cytoplasmic. In dermis, mononuclear inflammatory cells showed cytoplasmic staining with both antibodies. Granulocytes were negative with GRα, in contrast to strongly positive cytoplasmic staining with GRβ (Fig. 2). The location of the biopsy (upper arm or truncal skin) showed no difference.
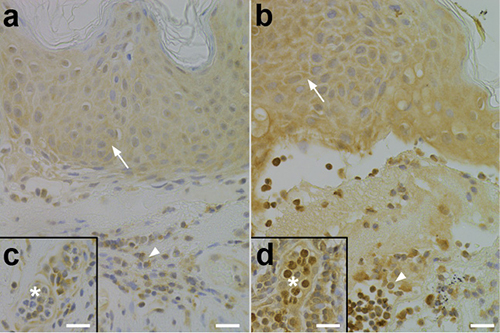
Fig. 2. Localization of glucocorticoid receptors (GR) in skin specimens. In epidermis, weak cytoplasmic staining with GRα antibody was detected (a; arrow), whereas GRβ staining was stronger (b; arrow). Mononuclear inflammatory cells showed cytoplasmic staining with both antibodies (a, b; arrowheads). Granulocytes were negative with GRα (c; asterisk) in contrast to strong staining with GRβ (d; asterisk). 40×; scale bar 20 μm.
Effect of prednisolone treatment on GRα and GRβ expression in bullous pemphigoid
To analyse the effect of systemic GC treatment on the expression of GR isoforms in BP, GRα and GRβ mRNA levels were measured from PBMC samples taken on days 5, 14 and 60 after the initiation of prednisolone. The analysis was conducted with 16 patients with BP (Table II). On day 5, GRα expression was up-regulated in 6 patients, down-regulated in 6 patients and remained unchanged in 2 patients (Table II). On day 14, the changes in GRα mRNA levels were variable: in 3 cases of BP the increase detected on day 5 continued; in contrast, in 4 cases the initial alteration had changed from decrease to increase, and in 5 cases, vice versa. Finally, on day 60, after 2 months of prednisolone treatment, the expression level of GRα was increased in 9 patients with BP, decreased in 4 and remained at the pre-treatment level in 1.
On day 5, the expression of GRβ was up-regulated or remained at the pre-treatment level in 12 patients with BP, and a decrease in the GRβ mRNA level was detected in only 2 cases (Table II). On day 14, the expression of GRβ remained increased in only 4 patients, but in 5 cases, the initial increase changed to a decrease. Interestingly, the prednisolone treatment promoted the expression of GRβ on day 5 or 14 in all 3 cases (BP3, BP11, BP15) in which GRβ mRNA was not detected in the pretreatment sample. At the end of follow-up, on day 60, the expression of GRβ was increased in 5 cases, remained at the pre-treatment level in 1 and was decreased in 7.
The mRNA expression levels of GRβ at different time-points were not statistically connected to GRα levels. The individual prednisolone dosages (mg/kg) at the time of the following sample had no statistical connection with GRα or GRβ mRNA expression levels.
DISCUSSION
This study demonstrates that the main GR isoforms, GRα and GRβ, are expressed in skin and PBMC samples of patients with BP. All BP and control samples showed expression of GRα mRNA in PBMCs, but GRβ mRNA expression was found in only a subgroup of them. GRα and GRβ protein expression was confirmed by FCM in all study subjects, but immunoblotting detected GRβ in only 4 out of 6 cases of BP. This may reflect the lower expression of GRβ compared with GRα and the sensitivity of the methods used. Immunohistochemical staining showed stronger immunostaining of keratinocytes and granulocytes with antibodies against GRβ than against GRα, an expected result based on previous studies (4). These results are, to a certain degree, comparable with our previous study of patients with severe atopic dermatitis (12), where we showed the expression of both GR isoforms in skin and PBMC samples.
Expression of GRα and GRβ was markedly changed after only 5 days of prednisolone treatment and continued fluctuating in many patients during the treatment period of 60 days. We expected to find a correlation between the long-term use of high prednisolone dosage and GR expression levels. Although the expression of GRβ was up-regulated on the 5th day of systemic GC treatment in the majority of patients with BP, the amount of GRβ varied randomly later on during the treatment. Up-regulation of GRβ expression has been shown to be induced very quickly after high doses of GCs (13), but the clinical relevance remains unclear in patients with BP.
In our study, none of the patients were considered totally GC insensitive, since all responded to GC
therapy. Due to worsening of symptoms, azathioprine was initiated as an adjuvant therapy for 3 patients with BP, but an increased amount of GRβ indicating GC insensitivity was not detected in their samples. Taken together, our current results indicate that the expression of GR isoforms varies greatly during prednisolone treatment, but the expression levels are not useful indicators of GC sensitivity in BP.
We also compared the expression of GR and clinical BP parameters. The BP180-ELISA values are used as a marker of disease activity (14). No correlation between BP180-ELISA values and GR isoform mRNA expression levels was observed (data not shown). In our study, the observation period was rather short (60 days), and therefore control BP180 values were not measured. Recently a novel tool, the Bullous Pemphigoid Disease Area Index (BPDAI), was proposed to be used to measure BP severity in clinical trials (15). However, our study was initiated before BPDAI was published, and, therefore, this index was not used. We should also take into account that the patients with BP, as well as the controls, were using several drugs and had several concomitant diseases (e.g. diabetes, Alzheimer’s disease), which act as confounding factors. However, as this was a real-life study, we did not wish to exclude any patients.
Before the era of GCs, BP was fatal in approximately one-third of cases (16). Systemic steroids are the best-evaluated treatment for BP (1). The proposed initial dosage of prednisolone is ≤ 0.5–0.6 mg/kg/day, but higher dosages are recommended for patients with severe clinical symptoms (17). Prednisolone doses > 0.5 mg/kg/day are well known to be associated with severe side-effects and heightened mortality (18, 19). In our study, the initial dosage of prednisolone was 0.38–0.69 mg/kg/day (mean 0.49 mg/kg/day), which is in line with the current recommendations. The dose of prednisolone did not correlate with GR isoform expression. This is in line with previous studies indicating that sensitivity to GC varies among individuals, and that even within the same individual, responsiveness to GCs differs among tissues and cells (20).
We conclude that patients with BP express both GR isoforms and their expression is altered during treatment with systemic GC. However, as our real-life study indicates, expression levels of GRα and GRβ as markers of steroid sensitivity are far from useful in clinical practice, at least in the elderly population and in patients with BP. More studies are needed to evaluate the safety of systemic steroid treatment and potential markers of steroid responsiveness.
ACKNOWLEDGEMENTS
The authors are grateful for the excellent technical assistance of Ms Anja Mattila, Ms Riitta Vuento and Ms Birgitta Grekula.
This work was supported by the Medical Research Center Oulu Doctoral Program, the Finnish Dermatological Society, the Finnish Medical Foundation, Väinö and Laina Kivi Foundation, Alma and K.A. Snellman Foundation and Foundation for Pediatric Research.
The authors declare no conflicts of interest.
REFERENCES

