


Departments of 1Dermatology and Allergology, 2Psychosomatic Medicine and Psychotherapy, University Clinic Giessen, 3Vitos-Clinic for Social Psychiatry, Department of Psychosomatics and Psychotherapy, Giessen, 4Special Hospital for Children and Adolescents Sylt/Westerland, and 5Institute of Medical Psychology, Justus-Liebig-University, Giessen, Germany
This study investigated the extent to which single mothers of children with atopic eczema experience disease-related stress. A total of 96 mothers were divided into 4 groups: mothers living with a partner, who had or did not have a child with atopic eczema, and single mothers, who had or did not have a child with atopic eczema. The following questionnaires were used to assess psychological burden: Short Stress Questionnaire (Kurzer Fragebogen zur Erfassung von Belastung; KFB), Satisfaction with Life Questionnaire (Fragebogen zur Lebenszufriedenheit; FLZ), General Depression Scale (Allgemeine Depressions-Skala; ADS), and the Questionnaire for Parents of Children with Atopic Eczema (Fragebogen für Eltern von Neurodermitis kranken Kindern; FEN). Single mothers had higher levels of helplessness and aggression due to their child’s scratching behaviour than did mothers living with a partner and a child with atopic eczema. Single mothers of children with atopic eczema had the highest scores regarding experienced stress in the family and the lowest scores concerning general life satisfaction. Special care should be provided for single mothers with higher stress, in order to teach them how to deal with the scratching behaviour of their children.
Key words: atopic eczema; atopic dermatitis; disease-related stress; single mother; depression; itch; scratch.
Accepted May 10, 2016; Epub ahead of print May 12, 2016
Acta Derm Venereol 2017; 97: 42–46.
Corr: Uwe Gieler, Department of Dermatology, University of Giessen, Gaffkystrasse 14, DE-35392 Giessen, Germany. E-mail: Uwe.Gieler@psycho.med.uni-giessen.de
A marked increase in atopic eczema (AE) has been observed in the past 2 decades (1, 2). In Germany, the reported risk of developing AE is approximately 12–15%. This skin disease is multifactorial in origin; both genetic disposition and psychosocial factors play a role in the onset and course of the disease. Everyday stressors and life events affect the condition of the skin (3). In children, conflicts within the family, in school and with friends have been observed in connection with a worsening of the state of the skin (4–7). Buske-Kirschbaum et al. (8) describe this relationship as a vicious circle. Stress can aggravate skin symptoms and thus further increase stress in patients with AE. This may lead to the maintenance and chronification of AE (9, 10). In another study it was shown that receiving maternal welfare in comparison to not receiving social welfare was associated with a higher risk to develop asthma (Odds ratio = 1.87; (11)). The social situation of being a single mother correlates with decreased well-being and increased health problems (12–14). This is relevant in determining the factors involved in the situation of single mothers with children with AE, since the number of single mothers is continually increasing in Germany. According to the Federal Bureau of Statistics in Wiesbaden (15), there were 2.7 million single parents in Germany in 2012 (out of a total population of 80 million), of whom 2.3 million were women.
The main aim of the study was to analyse whether the situation of single mothers with children with AE is different from that of mothers living in a family with children with AE. A further aim was to study whether the factor being a “single mother” affects coping with the child’s disease. Special attention was paid to life satisfaction, stress in everyday life and in the family, the emotional state and inclusion in a social network of single mothers with children with AE. In particular, it was of interest whether a combination of being a single mother AND of a child with atopic eczema compared to just being a single mother or a mother of a child with atopic eczema results in a significantly higher stress level. We hypothesized that single mothers of children with atopic eczema would display higher stress levels than mothers who only had a child with eczema OR were single.
A total of 145 mothers were invited to participate in the study, but 37 declined for different reasons, mainly time problems. The participation rate was therefore 74.5%. Data were collected from the 108 mothers in different locations (kindergarten, paediatric hospital, etc.). Only 96 of the total 108 data-sets were included in the final analyses, due to missing data and parallelization of samples. Inclusion criteria were: agreement to participate in the study; females in the age range 18–65 years; and having a child with AE diagnosed by a dermatologist or paediatrician. Exclusion criteria were: difficulty to understand German; unclear diagnosis, or if asthma was the most prominent diagnosis. Mothers with psychiatric diseases were also excluded.
The Short Stress Questionnaire (Kurzer Fragebogen zur Erfassung von Belastung; KFB) (16) measures non-health-related stress in 19 items. The Satisfaction with Life Questionnaire (Fragebogen zur Lebenszufriedenheit; FLZ) (17) examines satisfaction with life in 10 relevant areas (health, work and profession, financial situation, leisure-time, marriage and partnership, relationship with one’s children, self, sexuality, friends, acquaintances, relatives and living quarters). The General Depression Scale (Allgemeine Depressions-Skala; ADS) (18) offers a good diagnostic tool for currently-existing depressive symptoms in 20 items and is well-validated in international studies. The Questionnaire for Parents of Children with Atopic Eczema (Fragebogen für Eltern von Neurodermitis kranken Kindern; FEN) (19) was developed to determine the specific problems of parents whose children have AE with 22 items. The Questionnaire on Social Support (F-Sozu) developed by Fydrich & Sommer (20, 21) assesses individually-experienced social support/stress in 54 items. In all cases the German version of the questionnaires was used.
Data analysis was performed using SPSS program package 9.0 in 2005. The statistical procedures included: frequency counts, t-tests for independent samples and analyses of variance. Using an univariate analysis of covariance, the covariables age, education, severity and others were taken into account.
It was difficult to recruit single mothers with a child with AE; a final total of 16 were included. Sixteen single
mothers with healthy children were included after matching the sample for comparison. A total of 32 mothers with children with AE were included. All mothers agreed to participate in the study. These groups were then matched with 32 mothers living with partner or in a family with a healthy child. Table I presents the numbers of mothers included in each subgroup and the socio-demographic data for the subsamples.
Since the term “single mother” can be interpreted in different ways, we used the living conditions in the household. The groups were then divided into “living alone” and “living with a partner”. It was not regarded as important whether the partner was the child’s father, or whether the mother was married to the partner.
The mothers’ age range was 21–47 years, with a mean?±?standard deviation (SD) of 33.20?±?6.01 years, and showed a homogenous pattern. Differences regarding the severity of the child’s disease were recorded. Skin status (extent of involvement, reddening and itching) was examined by the mother. There were no differences between the children of mothers living alone or those living with a partner regarding skin status.
Comparison of single mothers and mothers living with a partner regarding stress (KFB) revealed a significant difference in perceived stress in the family and partnership, independent of the child’s state of health. There were no significant differences in the scales “Stress in Everyday Living”, “Social Relationships” and “Workplace” (see Table SI).
In addition, a significant difference regarding perceived stress in the family and partnership occurred, when mothers with children with AE and mothers with healthy children were compared. This was independent of the existence of a partnership. Here, too, there was no significant difference in the other 3 scales of the KFB (Table SI).
No significant interaction was found in this study between the two dimensions “partnership” and “child disease”. However, looking at the results for the scales of the KFB, overall single mothers of a child with AE reported the highest stress values.
Regarding overall satisfaction with life measured by FLZ, single mothers displayed significantly less satisfaction than mothers living with a partner, independent of the child’s state of health. In particular, single mothers were less satisfied with their financial state, their sexual life, their living quarters and their work and profession than mothers who were living with a partner (Table SI).
There was also a significant difference in “satisfaction with own health”. Mothers of children with AE were less satisfied with their health than mothers with healthy children, independent of the existence of a partnership.
No significant interaction effect occurred for “partnership” and “child disease” (Table SI).
The results measured with the General Depression Scale (ADS) showed a significant effect for “partnership” and “child disease”. Here, single mothers and mothers with a child with AE had higher scores. The interaction effect was not significant, but mothers with children with AE again had the highest values. The authors of the ADS define a score of less than 17 points as unremarkable. This score was exceeded only by the single mothers of children with AE.
The comparison of single mothers and mothers living with a partner, independent of the child’s state of health, revealed no difference in practical support with regard to the results of the F-SOZU-Questionnaire. However, there were significant differences between single mothers and mothers living in a partnership regarding support from the partner and acquaintances. Support from acquaintances was evaluated significantly higher by single mothers. There were no differences with regard to the child health. However, we found one significant interaction effect for the scale “instrumental support”. Mothers with a child with AE had the lowest values for “instrumental support”, whereas mothers living in a partnership and a child with AE had the highest values here.
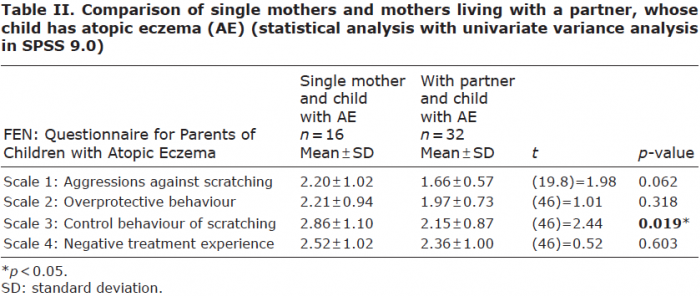
Moreover, we investigated whether mothers of children with AE cope differently with their child’s disease depending on the existence of a partnership. There was a significant difference between single mothers and mothers living with a partner regarding the scale “control behaviour of scratching”. Single mothers displayed more attention to the scratching behaviour than did mothers living with a partner. There were no significant differences in the scales “aggression against scratching”, “overprotective behaviour” and “negative treatment experience” (Table II).
This study detected fewer than expected significant differences in increased burden between single mothers with children with AE and single mothers without children with AE. However, there was a greater burden in single mothers regarding family and partnership compared with mothers living with a partner, independent of the child’s state of health. These results are in concordance with the results of Franz & Lensche (22), who consider the lack of an additional child-rearing partner as a very stressful factor.
Overall, life satisfaction in single mothers was also significantly lower than that of mothers living with a partner. Single mothers in comparison with mothers living with a partner were significantly less satisfied, especially in the sub-areas financial situation, sexuality, living quarters and work and profession.
Dissatisfaction regarding the socioeconomic situation and living quarters were also confirmed in other studies, e.g. by McLanahan & Booth (23), and Saul & Payne (24). The Federal Ministry of Labor and Social Order (15) published data in 2012 that showed that 65.2% of the single mothers they investigated had less than 50% of the median gross household income.
Contrary to our expectation, there was no difference in perceived social support between single mothers and mothers living with a partner, independent of the child’s state of health. However, single mothers reported receiving significantly more support from friends and acquaintances than did mothers living with a partner. The mothers living with a partner had significantly more support from the partner. The study results show that the social network of single mothers primarily consists of friends and acquaintances.
When comparing mothers of children with AE with mothers of healthy children, independent of the existence of partnership, it was found that the mothers of children with AE feel more burdened in the family and partnership than mothers of healthy children. Lawson et al. (25) found similar results. The parents of children with AE in their survey frequently reported experiencing exhaustion. Seventy-four percent of participants reported having additional household tasks that they had to perform. Sixty-six percent of the parents did not have the impression that they were able to live a normal family life, since there were many things in everyday life that they had to avoid because of their child’s disease. These included restrictions concerning diet or the use of cleansers. The higher risk in single mothers with children with AE to develop psychosomatic disorders was found by Pearlin & Johnson (26), and Baker & North (27). Mothers of children with AE reported significantly lower satisfaction with their state of health and also had a significantly higher score on the general depression scale than mothers living with a partner.
It was particularly interesting to determine whether the presence of a partner had a positive effect on coping with the child with AE. A significant difference was found in coping with the child’s scratching behaviour. In contrast to normal expectations, single mothers made significantly more attempts to control and prohibit their child’s scratching than did mothers living with a partner (see Table II). Single mothers reported a higher amount of control of scratching in the FEN, with a score of 2.86, in comparison with 2.15 for the mothers living with a partner and an atopic child. The child’s scratching behaviour also tends to elicit more aggression and helplessness among single mothers than among mothers living with a partner, even though no significant differences occurred between groups here. This could start a vicious circle. The increased attention from the mother conditions the continuance of scratching, leading to aggravation of events. The child experiences reward in attention from the mother and thus scratches even more (28). It would be better to react calmly to the child’s scratching or even to ignore it entirely (29, 30). The stress experienced by the mother is independent of the severity of the child’s AE and is related rather to her individual coping concepts. Other studies (25, 31) also found that parents of children with AE report higher levels of everyday stress. Moreover, the problems of the children regarding falling asleep as well as staying asleep, can lead to sleeping deficits and exhaustion in the parents. Many parents also report being under great emotional pressure and feel frustrated and helpless (32, 33).
The study has some limitations with regard to the small numbers of mothers in each group and the different numbers in the groups of single mothers and mothers living with a partner. The study was performed as a pilot study to generate hypotheses for further research, thus no high power was needed to test whether single mothers have higher severity of AE. A power calculation was not performed before the start of the study. Further research is needed on whether the age of the child, coordination with the other parent or partner who did not live in the same household, and the number of “other” adults in the household have an impact on life satisfaction or coping with eczema.
Thus far, most of studies on mothers of children with AE have not taken into account whether the mother was living with a partner or was raising the child by herself. Recent studies that have mentioned the situation of being a single mother or of the mother being in receipt of social aid have shown no statistically significant influence of this situation on AE (11, 33). Many authors point out the poor socioeconomic status of single mothers (23, 34). In addition to the often stressful financial situation, there is an increased incidence of mood fluctuations (35), depression and anxiety (27) among single mothers. Franz & Lensche (22) found a significant relationship between an increased emotional/psychosomatic impairment and lower satisfaction with income among single mothers. Moreover, they showed a lack of additional helpful others for the children of single mothers. A further reference person can be considered as an important support and might be a help for both the mother and the child, who can provide a protective factor for the child’s emotional and physical health.
There were not many highly significant differences regarding problems with children with AE when comparing single mothers and mothers with a partner and a child with AE. Although both show more stress than mothers of healthy children, the social situation seems to influence health behaviour more than AE. The limitations of this study are the small sample size and the cross-sectional design. Nevertheless, with respect to the established “atopic eczema education training for parents” (36, 37), this study shows that it is important to provide efficient information for single mothers regarding handling their children’s scratching behaviour and to support them by providing knowledge. Thus, a broader offer of practical assistance should be created for single mothers of children with AE. The goals should be to lower the stress level of single mothers and to reduce the conditioned scratching behaviour of the child.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize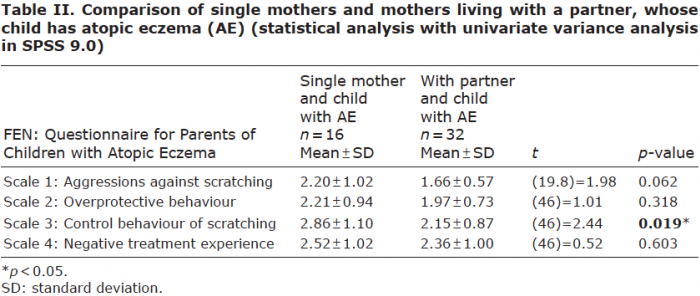 Click to show fullsize
Click to show fullsize