


Departments of 1Dermatology, Allergy, and Venereology, 3Obstetrics and Gynecology and 8Lübeck Institute of Experimental Dermatology (LIED),University of Lübeck, Ratzeburger Allee 160, DE-23538 Lübeck, Germany, 2Centre for Blistering Diseases, Department of Dermatology, University Medical Centre Groningen, University of Groningen, Groningen, The Netherlands, 4Department of Obstetrics and Gynecology, University Hospital Mannheim, Mannheim, 5Department of Dermatology, Venereology and Allergology, University Hospital Würzburg, Würzburg, 6Department of Dermatology and Allergology, Ludwig-Maximilian University, Munich, Germany, 7Department of Dermatology, Division of Immunology, Allergy and Infectious Diseases, Medical University of Vienna, Vienna, Austria. E-mail: Christian.Sadik@uni-luebeck.de
Accepted May 11, 2016; Epub ahead of print May 13, 2016
Pemphigoid gestationis (PG) is a pregnancy-associated blistering autoimmune skin disease, which most commonly erupts between the second trimester and the puerperium (1, 2). PG presents with pruritus and erythematous papules, urticarial erythema, and papulovesicles, as well as, in rare cases, blistering. Skin lesions predominantly arise initially on the periumbilical region. Onset of PG in the first or second trimester, as well as presence of blisters, are associated with adverse pregnancy outcomes (3). PG is driven by auto-antibodies directed to the hemidesmosomal adhesion molecule BP180. IgG auto-antibodies directed against the NC16A domain of BP180 can be found in 90% of patients with PG and, in some cases, remain positive after delivery (4–8). Auto-antibodies against a second hemidesmosomal protein, BP230, have been reported in up to 16% of PG sera (9), but the frequency of anti-BP230 auto-antibodies in healthy controls was not determined in this Japanese study. Detection of serum anti-BP180 NC16A IgG auto-antibodies by enzyme-linked immunoassay (ELISA) is the most convenient diagnostic method for PG. An alternative approach is the detection of auto-antibodies and complement at the dermoepidermal junction (DEJ) by direct immunofluorescence (DIF).
Recently, BIOCHIP® mosaic-based indirect IF microscopy has emerged as novel technique for the detection of skin protein-directed auto-antibodies in routine laboratory use (10, 11). Its validity for the diagnosis of PG, however, has not been investigated. Herein we report that detection of anti-BP180 auto-antibodies by BIOCHIP® mosaics is both highly sensitive and specific in discriminating patients with PG from healthy controls.
Sera from a total of 65 patients with PG were collected at the university hospitals of Lübeck (n = 14), Groningen (n = 26), Munich (LMU) (n = 10), Würzburg (n = 11) and Vienna (n = 4). Criteria for inclusion of patients with PG were a clinical presentation compatible with PG and a positive complement-binding test and/or anti-BP180 NC16A IgG enzyme-linked immunoassay (ELISA) results. Positive DIF microscopy results were not used as inclusion criterion, with DIF microscopy in clinical practice often avoided due to the requirement for skin biopsy. All clinical and laboratory details on the patients are summarized in Table SI. Sera from healthy para, taken in the first 24 h of the puerperium at the Department of Gynecology and Obstetrics, Lübeck, served as control (n = 102). All sera were stored between –80 and –20°C until use. The study was approved by the ethics committee of the University of Lübeck (12-178; 14-227).
All sera were subjected to the BIOCHIP® mosaic (Euroimmun, Lübeck, Germany) with 4 different substrates per incubation field, including primate split-skin, monkey oesophagus, recombinant tetrameric BP180 NC16A, and HEK293 cells expressing the C-terminal globular domain of BP230 (BP230 gC; amino acids 1875–2649) on the cell surface (10, 11). The BIOCHIP® mosaic assay specifically detects IgG auto-antibodies bound to the respective auto-antigens. Circulating anti-BP230 IgG auto-antibodies were determined in parallel by 2 different ELISA systems, using an E. coli-expressed fragment of the C-terminal globular domain of BP230 (Euroimmun; BP230-C; amino acids 2326–2649) and both the recombinant N- and C-terminal fragments (MBL, Nagoya, Japan; BP230-N-C; amino acids 1–979 and 1869–2649) (12, 13). All assays were performed according to the manufacturers’ instructions.
Data were analysed using GraphPad 7 software (GraphPad, San Diego, USA) and tested for statistical significance using Fisher’s exact test. p < 0.05 was defined as statistically significant.
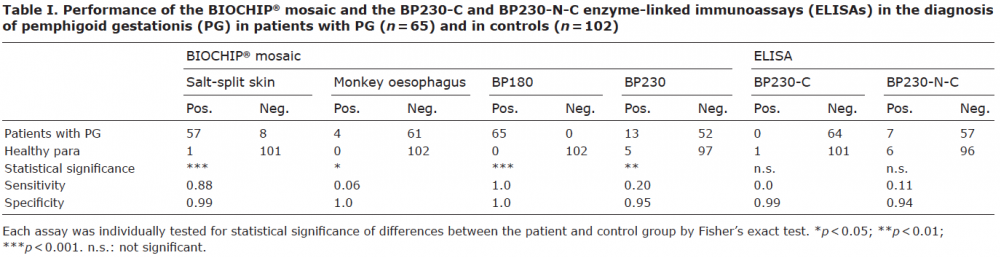
Sera from patients with PG and control para were screened for auto-antibodies using BIOCHIP® mosaics (Table I). In this assay, 57 (87%) sera from patients with PG were reactive on salt-split skin and 65 (100%) with BP180 NC16A. In the control group, only one (1%) serum was positive on salt-split skin and none of the sera contained anti-BP180 NC16A auto-antibodies (Table I). Thus, salt-split skin had a sensitivity of 0.88 and a specificity of 0.99 in distinguishing patients with PG from healthy controls, while detection of anti-BP180 auto-antibodies by BIOCHIP® mosaic resulted in the distinction of patients with PG and healthy controls with a sensitivity and specificity of 1.0. The BIOCHIP® mosaic detected anti-BP230 auto-antibodies in sera of 13 (20%) patients with PG and of 5 (5%) controls, a sensitivity of 0.20 and specificity of 0.95 (Table I). As the frequency of anti-BP230 auto-antibodies in patients with PG is still controversially debated, we also determined anti-BP230 auto-antibodies by the commercially available BP230-C and BP230-N-C ELISA sets. With the BP230-N-C ELISA, anti-BP230 reactivity was found in 7 (11%) PG sera and in 6 (6%) control sera, whereas in the BP230-C ELISA, none of the patients with PG and only 1 (1%) of the control samples were positive (Table I). Of note, none of the patient or control samples was positive in more than 1 of 3 assays for anti-BP230 auto-antibodies. Notably, when a positive DIF microscopy was used as mandatory inclusion criterion, the major results of our evaluation did not change (Table SII). A database search in Groningen and Lübeck identified 4 patients with PG with positive DIF microscopy and no reactivity for anti-BP180 auto-antibodies in the ELISA. Notably, all 4 patients were also negative for anti-BP230 auto-antibodies.
This study established the validity of the BIOCHIP® mosaic in the serological diagnosis of PG. The complete absence of anti-BP180 IgG auto-antibodies in healthy para is in line with previous reports on the frequency of anti-BP180 IgG auto-antibodies in healthy blood donors and in healthy pregnant women (14, 15), indicating that anti-BP180 NC16A IgG auto-antibodies do not emerge in healthy pregnancies. However, in some patients with PG, low titres of anti-BP180 auto-antibodies were detectable by ELISA, but mostly remained too low to reach the assay’s cut-off value (7). This phenomenon conceivably leads to falsely diagnosed cases of PG in patients who have had PG during a previous pregnancy, but who now have a different pregnancy-associated dermatosis, while still being anti-BP180 auto-antibody positive (7). Although we cannot fully exclude that our study included such patients, it is highly unlikely that these patients are more than a negligible percentage of the patients in this study.
Our results highlight the BIOCHIP® mosaic as an alternative to the complement-binding test and to anti-BP180 NC16A ELISAs. The general advantage of the BIOCHIP® mosaic is that it facilitates the usual multistep laboratory diagnostic of autoimmune blistering skin diseases into a single, easily to perform, assay. Furthermore, BIOCHIP® mosaic enables simultaneous screening for several auto-antibody species.
Although anti-BP230 auto-antibodies have been reported to be present in some patients with PG, the frequency of anti-BP230 auto-antibody formation in PG and its diagnostic and prognostic value have remained controversial. In our study, the percentage of anti-BP230 auto-antibody-positive individuals among both patients with PG and controls varied considerably depending on the immunoassay used and, when compared, the assays continuously delivered conflicting results. This discrepancy may be explained by the different BP230 fragments used as target structure in these assays. While the BP230-N-C ELISA detects anti-BP230 IgG antibodies directed against both the N- and C-terminal portions of BP230, the BP230-C ELISA only detects auto-antibodies against a small specific fraction of the C-terminal end. On the BIOCHIP®, in contrast, the entire globular C-terminal end of BP230, expressed in HEK293 cells, is presented (11). This notion is supported by the finding that none of the PG and control sera was positive for anti-BP230 antibodies in more than 1 assay system. Hence, all 3 anti-BP230 IgG assays must be considered to be of poor diagnostic value in PG, and positive anti-BP230 IgG auto-antibody results by either test must be interpreted with caution.
In summary, the BIOCHIP® mosaic can be used instead of the corresponding ELISA systems when absolute quantification of auto-antibody levels is not required. Furthermore, detection of anti-BP230 auto-antibodies does not add to the diagnosis of PG, when anti-BP180 and/or the complement-binding test are performed. By design, our study cannot exclude that the detection of anti-BP230 auto-antibodies may be instrumental in identifying a subgroup of patients with PG with typical clinical PG presentation and positive DIF microscopy, but without detectable levels of anti-BP180 auto-antibodies.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize