


Department of Dermatology, Shiga University of Medical Science, Setatsukinowa, Otsu, Shiga 520-2192, Japan. E-mail: kihsekat@belle.shiga-med.ac.jp
#These authors contributed equally to this work.
Accepted May 16, 2016; Epub ahead of print May 27, 2016
Necrotizing fasciitis (NF) is a fatal disease that warrants immediate diagnosis and surgical debridement. However, it is difficult to differentiate NF and cellulitis at the first visit, since the clinical presentation of both disease entities appears similar in the early phase. The availability of the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score to diagnose NF was proposed by Wong et al. in 2004 (1). They compared a set of laboratory risk indicators between NF and other soft tissue infections. The total score of the LRINEC ranges from 0 to 13, and the cut off score of 6 was found to have a positive predictive value of 92% and a negative predictive value of 96%.
Procalcitonin (PCT) is a peptide precursor of the hormone calcitonin, which is involved in calcium homeostasis. The level of PCT increases in response to a proinflammatory stimulus, especially of bacterial origin (2). During a bacterial infection, PCT is produced mainly by the cells of the lungs and intestines, which is a reliable marker in the diagnosis and treatment of serious bacterial infections and sepsis (3). Therefore, we measured the level of PCT in NF and cellulitis in order to evaluate whether its usefulness for early discrimination between the 2 conditions as compared to LRINEC and creatine kinase (CK) levels in blood.
A retrospective review of 3 patients with NF and 21 patients with cellulitis, who were hospitalized in the Department of Dermatology in Shiga University of Medical Science, Shiga, Japan, between September 2010 and February 2014, was conducted. Since the study was performed retrospectively in a single centre, institutional review board approval was not required. Data were extracted from hospital records. In this study, NF was confirmed by operative exploration in all cases. White blood cell count (WBC), C-reactive protein (CRP), CK, LRINEC score, and PCT were registered. Serum PCT was measured by VIDAS 30 and VIDAS B·R·A·H·M·S PCT (Sysmex-bioMérieux Japan, Kobe, Japan). In the group of patients with NF, PCT were examined on the day of acute admission (Cases 1 and 3) or 3 days after acute admission (Case 2). During the first 2 weeks after admission, PCT levels were measured 3 times (Case 1), 2 times (Case 2), and 9 times (Case 3), respectively. In the group of patients with cellulitis, the average day to measure PCT levels after admission was one day. In most cases, the PCT assay was performed only once and the mean number of measuring times was 1.19. We calculated the sensitivity, specificity, positive predictive value, and negative predictive value of the LRINEC score and evaluated its appropriateness. Moreover, we analysed the correlation between the level of PCT and NF or cellulitis using a t-test.
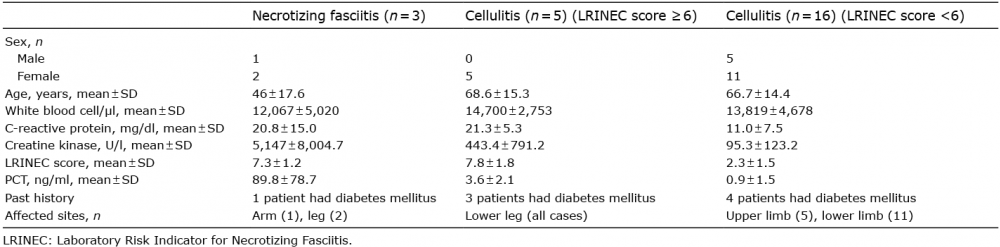
Table SI shows the characteristics of 3 cases of NF and 21 cases of cellulitis. In all cases, the levels of PCT decreased after treatment. All patients with NF had LRINEC scores 6–8. Among the patients with cellulitis, there were 5 cases with a LRINEC score ≥ 6 and 16 with a LRINEC score < 6. As summarized in Table I, the level of CK in 3 cases of NF was significantly higher compared with the 21 cases of cellulitis (p = 0.0033). The cut-off point to differentiate NF and cellulitis by using receiver operating characteristic (ROC) curve analysis was 534.5 U/l. With this cut-off point, the CK level has 66.7% sensitivity, 95.2% specificity, 66.7% positive predictive value, and 95.2% negative predictive value. A LRINEC score of ≥ 6 as a predictive marker for NF, showed 100% sensitivity, 76.2% specificity, 37.5% positive predictive value, and 100% negative predictive value. Lastly, the PCT level in the 3 cases of NF was higher than in the 21 cases of cellulitis (p < 0.0001). Statistical difference was also observed when the 3 cases of NF and 5 cases of cellulitis with a LRINEC score ≥ 6 were compared (p = 0.0409). Even when we set the cut-off point in the range of 5.88 to 19.96, the PCT level has 100% sensitivity, 100% specificity, 100% positive predictive value, and 100% negative predictive value in distinguishing NF from cellulitis.
Table I. Summary of clinical and laboratory characteristics in necrotizing fasciitis, and in cellulitis with LRINEC scores of ≥ 6 and <6
Nakafusa et al. (4) reported that serum CK level is important as a prognostic factor in Vibrio vulnificus infection. In our study, the level of CK in the cases of NF was significantly higher compared with the cases of cellulitis, but the cut-off point that we established had lower sensitivity than the LRINEC score, and PCT value. One possible reason for this low sensitivity is that the elevation of CK level in NF seems to depend on the types of causative bacteria. Simonart et al. (5) reported that the majority of NF patients with group A β-haemolytic streptococci as the causative agent had elevated CK values early in the course of their disease, while most patients with other bacteria exhibited CK values within normal ranges (5). In our study, Cases 1 and 2 had group A β-haemolytic Streptococcus (S.) pyogenes, and Case 3 has group G S. dysgalactiae subsp. equisimilis. From these results, the CK level is not reliable for early discrimination between NF and cellulitis.
After Wong et al’s. (1) proposal that the LRINEC scoring is capable of detecting early cases of NF, several other studies have reported the usefulness of the LRINEC score (6–8). However, the validity of LRINEC scoring is still debatable. Indeed, when we evaluate our 24 cases using LRINEC score, the 3 cases of NF are diagnosed properly, whereas 5 cases of cellulitis are misdiagnosed as NF. Although the LRINEC score of NF is usually higher than that of cellulitis, in Cases 4 and 5, the reverse is true (see Table SI). These results indicate that LRINEC scoring can lead to overdiagnosis in spite of its excellent sensitivity for NF.
Interestingly, the PCT level was significantly higher in NF than in cellulitis. Nylén et al. (9) reported already in 1992 that the level of PCT increased in burn patients. According to Schuetz et al. (10), the cut-off value of PCT to determine the need for antibiotics is 0.10 ng/ml. From our study, we can set the cut-off point in the range 5.88–19.96 to have 100% sensitivity, 100% specificity, 100% positive predictive value and 100% negative predictive value in distinguishing NF from cellulitis. However, the level of PCT is elevated due to many causes, including bacterial infection, severe mechanical trauma, severe burns, inflammation associated with cytokine storms, and so on (11). Although sepsis was present in 2 cases of cellulitis (Cases 6 and 13) and all cases of NF, the level of PCT in NF is obviously higher than in the former 2 cases.
In conclusion, the level of PCT was significantly higher in cases of NF than in cases of cellulitis in this study. Al-though only a limited numbers of patients were examined by us, this is the first report showing the usefulness of PCT in the early diagnosis of NF. Further investigation is needed in order to determine an adequate cut-off point of PCT for discriminating NF from cellulitis.
Nakafusa et al. (4) reported that serum CK level is important as a prognostic factor in Vibrio vulnificus infection. In our study, the level of CK in the cases of NF was significantly higher compared with the cases of cellulitis, but the cut-off point that we established had lower sensitivity than the LRINEC score, and PCT value. One possible reason for this low sensitivity is that the elevation of CK level in NF seems to depend on the types of causative bacteria. Simonart et al. (5) reported that the majority of NF patients with group A β-haemolytic streptococci as the causative agent had elevated CK values early in the course of their disease, while most patients with other bacteria exhibited CK values within normal ranges (5). In our study, Cases 1 and 2 had group A β-haemolytic Streptococcus (S.) pyogenes, and Case 3 has group G S. dysgalactiae subsp. equisimilis. From these results, the CK level is not reliable for early discrimination between NF and cellulitis.
After Wong et al’s. (1) proposal that the LRINEC scoring is capable of detecting early cases of NF, several other studies have reported the usefulness of the LRINEC score (6–8). However, the validity of LRINEC scoring is still debatable. Indeed, when we evaluate our 24 cases using LRINEC score, the 3 cases of NF are diagnosed properly, whereas 5 cases of cellulitis are misdiagnosed as NF. Although the LRINEC score of NF is usually higher than that of cellulitis, in Cases 4 and 5, the reverse is true (see Table SI). These results indicate that LRINEC scoring can lead to overdiagnosis in spite of its excellent sensitivity for NF.
Interestingly, the PCT level was significantly higher in NF than in cellulitis. Nylén et al. (9) reported already in 1992 that the level of PCT increased in burn patients. According to Schuetz et al. (10), the cut-off value of PCT to determine the need for antibiotics is 0.10 ng/ml. From our study, we can set the cut-off point in the range 5.88–19.96 to have 100% sensitivity, 100% specificity, 100% positive predictive value and 100% negative predictive value in distinguishing NF from cellulitis. However, the level of PCT is elevated due to many causes, including bacterial infection, severe mechanical trauma, severe burns, inflammation associated with cytokine storms, and so on (11). Although sepsis was present in 2 cases of cellulitis (Cases 6 and 13) and all cases of NF, the level of PCT in NF is obviously higher than in the former 2 cases.
In conclusion, the level of PCT was significantly higher in cases of NF than in cases of cellulitis in this study. Al-though only a limited numbers of patients were examined by us, this is the first report showing the usefulness of PCT in the early diagnosis of NF. Further investigation is needed in order to determine an adequate cut-off point of PCT for discriminating NF from cellulitis.


 Click to show fullsize
Click to show fullsize