


Department of Dermatology, Medical School, University of São Paulo, Rua Itapeva 500, 3ºA, São Paulo, Brazil. *E-mail: mentanico@hotmail.com
A 60-year-old circumcised man presented with an asymptomatic lesion on his glans penis, which had been present for 2 years. He had been circumcised in adolescence, possibly due to phymosis. Clinical examination revealed areas of thick, stratified and adherent keratosis, surrounded by a silvery, scaly and slightly atrophic plaque over the glans penis and around the urethral meatus (Fig. 1). No adenopathy was palpable, and the patient was in good health. Topical therapies with emollients and corticosteroids (betamethasone valerate, clobetasol) had been tried, with no success.
Fig. 1. Adherent, intensely keratotic lesions over a silvery scaly patch on the glans penis.
A biopsy was taken from the thick keratotic portion. Histopathology revealed marked hyperkeratosis with focal parakeratosis, extensive acanthosis with only slight atypia of the lower epidermal layers. The dermis showed mild lymphocytic infiltrate (Fig. 2).
Fig. 2. Biopsy from a keratotic lesion showing marked hyperkeratosis and acanthosis with slight basal atypia. (Haematoxylin and eosin, ×150).
What is your diagnosis?
Diagnosis: Pseudoepitheliomatous, keratotic, and micaceous balanitis (PKMB)
Pseudoepitheliomatous, keratotic, and micaceous balanitis (PKMB) was first named and described by Lortat-Jacob & Civatte in 1961 in the French literature and by Bart & Kopf in 1977 in the English literature (1). Most recent reports come from India (1–4). The exact nature of this chronic condition is not known; it possibly represents a common clinical presentation, or association of distinct disease processes, mostly lichen sclerosus and atrophicus, and verrucous carcinoma (2, 5). PKMB is very rare; there are no published case series, only individual case reports. Patients are usually older men who have undergone circumcision in adulthood; however, uncircumcised men may very rarely develop similar symptoms (6). Previously excised penile tumours can relapse with a clinical aspect of PKMB (7).
Clinically, PKMB presents as a chronic, non-inflammatory lesion, which takes on a silvery white appearance; characteristic mica-like and adherent keratotic horny masses are seen on the glans. Some authors refer to “nail-like growths”. The keratotic scaling is usually micaceous and may resemble psoriasis. Rarely, erosions, cracking and fissuring crusts are present, as well as meatal constriction. Progressive thickening, with consequent destruction of deeper tissues, may develop (verrucous or invasive carcinoma) (3, 4).
Histological features of PKMB depend on the underlying process, and most often reveal intense acanthosis, hyperkeratosis, and epithelial hyperplasia with no or only slight cytological atypia (6). Dermal infiltrate is usually scarce. These features were present in our case, and may be those of a very well differentiated superficial verrucous carcinoma.
Differential diagnoses of PKMB include psoriasis, lichen sclerosus et atrophicus, viral warts, and other clinical types of squamous cell carcinoma.
Therapeutic modalities described include topical 5-fluoracil (2), cryotherapy, photodynamic therapy (5) and surgical excision (4).
Since, in most cases, PKMB seems to represent a presentation of squamous cell carcinoma, strict long-term follow-up is warranted (8).
The case reported here fulfils all the clinical and histological criteria for PKMB; however, we believe that this diagnosis is purely morphological; the exact nature of the process should always be determined in a given case, in order to determine the best treatment and prognosis.


 Click to show fullsize
Click to show fullsize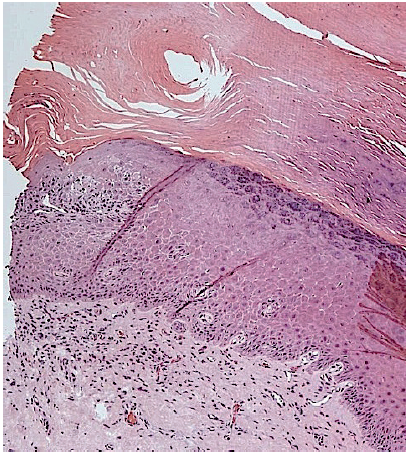 Click to show fullsize
Click to show fullsize