


1Institute of Psychology, University of Silesia, Katowice, 2SWPS University of Social Sciences and Humanities, 3The Cardinal Stefan Wyszy?ski Institute of Cardiology, Warsaw, and 4Department of Dermatology, Medical University of Silesia, Katowice, Poland
The aim of this study was to examine the importance of psychosocial factors, such as emotional and instrumental social support, distress, and assumptions about appearance and its salience to one’s self-worth, and to relate these factors to depressive symptoms in patients with psoriasis, according to gender. A group of 219 patients with psoriasis, aged 18–70 years completed the Beck Depression Inventory, the Appearance Schemas Inventory-Revised, the Berlin Social Support Scales, and the Distress Thermometer. Body Surface Area index was used to assess the severity of psoriasis. The main contributors to depression were: female gender, beliefs about appearance and its salience to one’s self-worth, greater psychological distress, and lower levels of emotional social support. Therefore, improving the body image of patients with psoriasis, by reducing its salience in their personal lives, may play a role in the prevention of depression, especially in women.
Key words: psoriasis; depression; distress; body image; social support; gender.
Accepted Jun 1, 2016; Epub ahead of print Jun 15, 2016
Acta Derm Venereol 2017; 97: 91–97.
Corr: Ewa Wojtyna, Institute of Psychology, University of Silesia, ul. Gra?y?skiego 53, PL-40-126 Katowice, Poland. E-mail: ewa.wojtyna@us.edu.pl
Psoriasis is one of the most common immune-mediated inflammatory skin diseases, with an estimated prevalence of 2–3% of the Caucasian population worldwide (1). Psoriasis can occur at any age and is equally distributed between men and women. As with other skin diseases, visible disfigurement triggers negative reactions in others, which can cause much of the readily measurable psychosocial burden of the disease. However, the impact of psoriasis on patients’ lives and well-being is often higher than in other skin and chronic diseases (2–4). To date, extensive literature describes the co-occurrence of psoriasis and depression, suicide ideation, anxiety, sexual dysfunction and alcohol addiction (2, 5–9). Physical, psychological and socioeconomic burdens of psoriasis include skin discomfort, disfiguration, feelings of stigmatization, and inconvenient and uncomfortable skin therapies. These burdens may lead to negative affect (in particular sadness, loneliness, and anger), may strongly influence body image, and may eventually result in negative mental health outcomes (10–15).
It has also been reported that women with psoriasis might incur a higher risk for psychological comorbidities than do men (14, 16–18). Thus, gender differences in the impact of psoriasis are an important issue. It is worth noting that appearance norms directed at women are more rigid, homogeneous, and pervasive than are those directed at men (19), which may exacerbate existing psychological distress and negative body image.
It should also be emphasized that the psychological impact of psoriasis may be highly individual and often not in proportion to the clinical severity of the disease, or to the extent and the location of skin lesions (9, 20–22). In many patients, the physical psoriasis score may not reflect the level of psychosocial disability (9, 23, 24). Psychological impairments in psoriasis might be largely attributable to patients’ perception of the disease (e.g. 20, 24–26) and/or beliefs about the importance of appearance in one’s personal life and its salience to a sense of self-esteem (e.g. 27–29). Furthermore, perceived social support and positive, acceptable experiences of social interactions may be of particular importance for this group of patients. However, social support can have different effects depending on the gender of the recipient and the match between the type of social support and the individual’s needs (18, 30). For example, Janowski et al. (18) found that social support might generally be more effective in preventing depression in women than in men with psoriasis. Less is known about the protective effects of different types of social support and potential gender differences in the links between social support and mental health among patients with psoriasis. Types of social support and gender have rarely been controlled factors in such studies; therefore, they are important issues to consider.
The aims of this study were to describe the severity of depression and distress in patients with psoriasis in Poland, and to determine factors associated with depressive symptoms. Selected factors, such as gender, age at onset of psoriasis, extent of the disease, perceived social support, and other psychological variables, were investigated. These variables included subjective distress, and beliefs about the importance and influence of appearance in the patient’s life, which could account for increased probability of co-occurrence of psoriasis and depression.
A descriptive cross-sectional study was conducted among patients with psoriasis. Survey invitation letters were sent to dermatology outpatient and inpatient clinics, and to Polish psoriasis associations. Ethical approval was granted by the Ethics Committee of the University of Silesia.
Inclusion criteria were: psoriasis diagnosed by a dermatologist; at least one year disease duration; age ≥ 18 years; no physical disfigurement unrelated to psoriasis; no serious mental or cognitive disturbances; and informed consent.
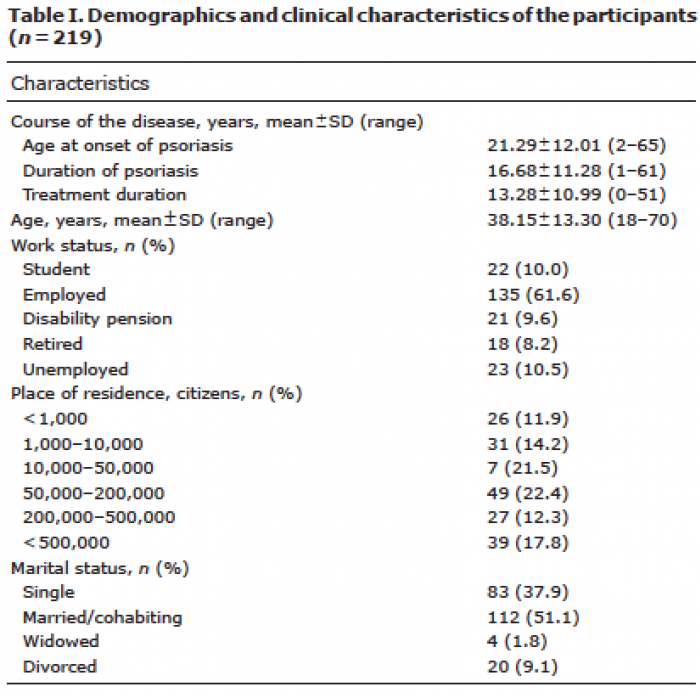
The final sample comprised 219 patients: 124 women (56.6%) and 95 men (43.4%). The baseline characteristics of the sample are shown in Table I.
Table I. Demographics and clinical characteristics of the participants (n = 219)
Beck Depression Inventory (BDI). The BDI is one of the most widely used self-report measures of depression, with high validity and good psychometric properties (31, 32). The 21-item questionnaire uses a 4-point response scale (0 = low, 3 = high). Scores on the 21 items corresponding to the symptoms of depression are summed to give a single total score, ranging from 0 to 63. Higher total scores indicate more severe depressive symptoms. Scores in the range 0–13 indicate lack or minimal depression, 14–19 mild depression, 20–28 moderate depression, and 29–63 severe depression. A validated Polish version of the BDI was used in the current study (33). Cronbach’s α coefficient for the BDI is 0.91.
Appearance Schemas Inventory – Revised (ASI-R). The ASI-R is a 20-item, Likert-type instrument assessing body image investment as reflected in beliefs about the importance and influence of appearance in one’s life (34). The ASI-R comprises 2 subscales: Self-Evaluative Salience (SES; 12 items), which assesses the extent to which individuals define themselves and their self-worth by their physical appearance, regarded as influential in their social and emotional experiences; and Motivational Salience (MS; 8 items), which measures attention to appearance, and performance of appearance-management behaviours. In the study reported here the Cronbach’s α coefficient amounted to 0.88 for the general score, 0.89 for SES, and 0.86 for MS.
Berlin Social Support Scales (BSSS). The BSSS (35, 36) are multidimensional measures of social support. One of the 6 BSSS scales was used in the present study: Perceived Available Support (including perceived emotional and instrumental support). Each of 8 items is rated on a scale from 1 (strongly disagree) to 4 (strongly agree). The BSSS has demonstrated good internal consistency and validity (35, 36). In the study reported here the Cronbach’s α coefficient amounted to 0.90 for the Perceived Available Support, 0.93 for Emotional Support Subscale, and 0.88 for Instrumental Support Subscale.
Body Surface Area (BSA). The BSA index was used to assess the extent of psoriasis. BSA is a simple and commonly used instrument for measuring the percentage of body surface area affected by psoriasis (16, 37). Mild involvement of skin with psoriasis was defined as 1–10% BSA; moderate to severe involvement as >10% BSA (38).
Distress Thermometer (DT). The DT (39) was used to assess the level of distress in patients with psoriasis. The DT is a visual analogue scale that looks like a thermometer and ranges from 0 (no distress) to 10 (extreme distress). Patients were instructed to place a horizontal line at the number corresponding to the level of recently experienced distress. Results of the validation study of the Polish version of the DT indicated that scores ≥ 4 have been associated with increased risk for anxiety and depressive disorders.
Data were analysed using the statistical package STATISTICA 12 (StatSoft Inc.). A t-test was used for group comparisons. Effect sizes (Cohen’s d) were also estimated and reported. Stepwise multiple regression analyses were used to indicate predictors of depressive symptoms in the total sample, and in men and in women separately. Multivariate logistic regression analysis was performed to describe factors associated with the likelihood of depression.
More than half of the participants (69.4%) reported distress score ≥ 4 on the DT.
The mean ± standard deviation level of depressive symptoms, as measured by BDI (14.18 ± 11.41), were within the score range indicative of clinical depression (Table II). Almost half of the participants (49.8%) fell into the category of probable depression; among those, 11.9% presented severe, 18.2% moderate and 19.7% mild depressive symptoms, as defined by the BDI. Moreover, nearly 21% of respondents in our sample reported suicidal thoughts.
Depressive symptoms and distress were significantly higher in women than in men (Table II). Moreover, women also reported more self-evaluative investment in their appearance, and significantly greater levels of motivational salience.
Table II. Differences between women and men with psoriasis on depression, distress, body image, social support and extent of the disease
As Table III shows, self-evaluative salience, distress, emotional social support, and extent of the disease made significant contributions to the variance in depression in patients with psoriasis. The total variance of all entered variables was 0.49 (adjusted R2). The main contributors to depression were distress and emotional social support. Distress accounted for over 29% of the variance, and emotional social support accounted for a further 15% (Table III). The extent of the disease (BSA) accounted for a modest proportion of the variance, and did not make a significant contribution to the variance in depression in women (Table III). In contrast, for women, the importance of appearance in their personal life and its salience to their sense of self emerged as a significant predictor, contributing 5% to the variance in depression.
Table III. Predictors of depression in patients with psoriasis
In addition, multivariate logistic regression revealed that female gender was an important risk factor for depressive symptoms (odds ratio [OR] 2.36). For women, the risk for depression was more than double that for men (Table IV). High levels of psychological distress (distress ≥ 4 on the DT) quadrupled the chances of depression in psoriasis patients (OR 4.17). Moreover, the importance of physical appearance in personal life and its salience to the sense of self and esteem were associated with a more than 4-fold increased risk of having depressive symptoms (OR 4.46). Analysis also revealed that emotional support was the most important protective factor for depression (OR 0.20). The instrumental social support variable did not reach statistical significance.
Table IV. Risk factors associated with depression in
patients with psoriasis (n = 219)
One of our research objectives was to determine the levels of psychological distress and depressive symptoms in Polish patients with psoriasis. Overall, and consistent with current knowledge, our results show high rates (nearly 50%) of comorbid depression in patients with psoriasis (2, 6, 7). High levels of psychological distress were present in 70% of patients. This is an important issue, because psychiatric disorders have been found to be associated with poor treatment adherence, poor therapeutic response, and inferior outcome in patients with psoriasis (40–42) and, furthermore, are an additional source of suffering and disability. Moreover, as recently reported by other authors, depression, and especially acute depression, in patients with psoriasis is associated with increased risk of myocardial infarction, stroke, and cardiovascular death (43).
Our results also show, consistent with what has been previously reported by other authors (16, 18), that women were more prone to depressive symptoms and psychological distress. Women also reported stronger beliefs about the importance and influence of physical appearance on their personal or social worth and significantly greater levels of motivational investment in their appearance. Interestingly, the extent of psoriasis was unrelated to the risk of depression in women, and was a statistically significant, but weak, determinant of depressive symptoms in men. This result is in agreement with previous research (9, 16, 20, 18, 44), in which the severity of psoriasis was weakly or not significantly associated with the degree of deterioration in mental health and quality of life. It has also been reported (23, 24) that physical measures of disease severity, such as the PASI or BSA, give only a partial indication of psychosocial disability caused by psoriasis, and the impact of psoriasis beyond the skin often goes unrecognized or is undertreated (45, 46). We observed, however, that the impact of psoriasis seems to be different in women and men. The results of this study suggest a direct effect of psoriasis on depressive symptoms in men. In contrast, for women the extent of the disease was unrelated to depression, but a significant contributor to depression was the importance of physical appearance in one’s personal life and its salience to one’s sense of self and esteem. Thus, our results suggest that, in women, cognitive factors related to aspects of body image may serve as a mediator between psoriasis and negative mental health outcomes. However, further research is needed to verify this assumption.
Understanding the key risk factors of impairment may help physicians to identify patients who are more vulnerable to the negative impact of psoriasis and to make more appropriate treatment decisions earlier in the course of disease (e.g. to implement a multifaceted intervention), potentially preventing the progression of cumulative impact of the disease. The impact of psoriasis seems to be highly individual, and not in proportion to the severity of the disease (9). According to our results, a possible reason underlying the high prevalence of depression in patients with psoriasis might be an overemphasis on appearance in the evaluation of self-worth. Dysfunctional schematic investment in one’s appearance may strongly trigger disease-related burdens, especially in women. Psoriasis is a disease closely related to concerns about appearance. Moreover, women are more frequently valued and assessed by their appearance than are men. Appearance norms directed at women are also more rigid, homogeneous and pervasive than are those for men (19). Therefore, women with a greater self-evaluative salience of their appearance might be particularly predisposed to body image dissatisfaction, which may exacerbate psychological distress, and consequently increase risk of depression. In contrast, in men, self-evaluative salience of appearance did not seem to play a role in depressive symptoms. However, we detected other risk factors for depression in both genders. Psychological distress was an important risk factor for depression both in men and in women. This result is in line with a previous report (22), suggesting that patients with high subjective distress, regardless of disease severity, should be evaluated for depression.
Moreover, according to our results, higher levels of perceived emotional social support were positively linked to lower depressive symptoms. Emotional support was the most important protective factor for depression in psoriasis patients; however, this relationship was considerably more significant in women. But, contrary to our expectations, there was no significant association between instrumental social support and depression. We hypothesize that the role of instrumental social support may be more complex, because this type of support may make patients feel less in control of their situation, decrease the controllability of the disease and enhance helplessness. There is little evidence for a mental health benefit from the various types of social support to patients with psoriasis. However, Janowski et al. (18) reported that higher tangible support was the strongest predictor of lower depressive symptoms in patients with psoriasis, and that other social support dimensions did not reach significance. In line with our outcomes, they stated that social support may be viewed as a buffer for emotional disturbances revealed in the form of depressive symptomatology in women, whereas this effect may be less important for men. Further research is needed before strong conclusions can be made regarding the protective effects of various social supports on mental health in patients with psoriasis.
As mentioned earlier, in this study, clinical characteristics of psoriasis, such as extent of the disease, had poor predictive value for depression. Localization of skin lesions and clinical history variables, such as age at onset, did not reach statistical significance. In contrast, Remröd et al. (47) found that patients with early-onset psoriasis (age < 20 years) were significantly more depressed and anxious than were patients with late onset of the disease. However, there is still little information available on the link between childhood onset of psoriasis and mental health in adulthood. Early-onset psoriasis has the potential to change the patient’s life trajectory substantially (15, 48) and may be an important, but not essential, risk factor for depression in patients with psoriasis. Moreover, our results might best be viewed in light of the cognitive-behavioural importance of appearance in one’s personal life. In this study, 72.1% of participants were between 18 and 45 years old; therefore, it is safe to assume that their beliefs and attitudes toward the body are the result of cultural changes that have occurred in the past 5–10 years, especially a societal focus on beauty and the notion of the “perfect body”, as is often conveyed in modern mass media. Accordingly, our results indicate that maladaptive beliefs about physical appearance and its salience to one’s life and self-worth are important risk factors for depression (especially in women). However, this relationship may be considerably more complex than it first appears. Paradoxically, in patients with severe psoriasis, a more severe condition may have the effect of reducing their investment in appearance and its salience to their lives. Patients with more severe disease may feel exempt from societal standards and cultural expectations of the perfect body, and may be able to develop consistent and effective ways of coping. In contrast, individuals with mild skin lesions may be more likely to feel pressured to meet ideals of physical appearance, and, among these individuals, body image investment reflected in beliefs about the importance of appearance in one’s life and self-worth can be a major contributor to negative mental health outcomes. Thus, psychological impairments associated with psoriasis may be largely attributable to patients’ maladaptive assumptions about physical appearance and society’s focus on beauty and the perfect body, rather than to the age of onset of psoriasis. Further research is are needed to test these assumptions.
In our study, the presence of psoriatic lesions on the face or genital skin did not have a significant association with depressive symptoms. These results are contrary to previous research (22), where the presence of genital lesions was clearly linked to depression. Nevertheless, other authors have suggested that the psychological burden of psoriasis might be largely attributable to the mere fact of having psoriasis and the patient’s own perception of the disease and/or other psychological factors, rather than to physical characteristics of psoriasis, such as severity, localization of skin lesions, and clinical history variables, such as family history, duration, and age at onset (18, 20, 49). For example, Hrechorów et al. (49) found that the presence of psoriatic lesions on the face had no influence on patients’ feelings of stigmatization, even though patients with facial lesions had significantly more severe psoriasis and the face is the most visible area of the body. Future studies should pay more attention to the associations between depression and the presence of psoriatic lesions on readily visible and “emotionally charged” body regions, such as face, hands, and/or genitals, vs. body areas that can be covered more easily. In addition, further research is required to better determine the link between childhood onset of psoriasis and mental health in adulthood.
To our knowledge, this is the first study to evaluate the role of psoriasis patients’ assumptions about physical appearance and its salience to their life and self-worth as a risk factor for depression. However, this study has some limitations that should be taken into consideration when interpreting the results. First, our sample included participants from psoriasis associations, which may limit the generalizability of the results. Members of such associations may have (by the very fact of their membership) considerable concern regarding their disease and, possibly, greater psychosocial burden of psoriasis. Secondly, the study was cross-sectional in nature, and so has all the disadvantages of cross-sectional studies (e.g. one cannot determine the sequence of events). Therefore, prospective replication is necessary to confirm the results. Thirdly, as in previous studies (16, 22, 37), the extent of psoriasis was assessed according to BSA. This measure enables one to define the body surface area affected by psoriasis, but is not a complete assessment of severity. BSA does not estimate other clinical signs, such as erythema, induration, and desquamation. Future research could extend the current findings by taking into account the assessment of psoriasis severity measured both by the physician and by the patient’s self-report.
Moreover, our results showed, consistent with others’ reports (18), that women with psoriasis were more prone to depressive symptoms than were men. National population surveys have also consistently shown a higher prevalence of depression in women than men (50, 51). However, gender is likely to play an important role in how men and women conceptualize and experience depression (52, 53). The large gap in depression rates between men and women may be strongly affected by individuals’ adherence to socially constructed gender role norms. Women may see depression as a socially acceptable reaction to visible disfigurement and be more likely than men to endorse the internalizing symptoms that are consistent with standard DSM-5 diagnostic criteria. Men may be more likely than women to manifest externalizing symptoms (e.g. irritability, aggression, substance/alcohol abuse) not included in a standard evaluation for a depressive disorder. Therefore, the higher prevalence of depression in women may be an artefactual finding. According to Martin et al. (52) and Genuchi & Mitsunaga (53), when externalizing symptoms are included in the assessment of depression, the gender differences in overall symptoms disappear. Thus, further research is necessary, using a measure that includes both internalizing and externalizing depressive symptoms, to understand gender differences in the co-occurrence of psoriasis and depression.
High rates of psychological impairments were found in patients with psoriasis in Poland. The results indicate the importance of early diagnosis of psychological burden of the disease and a great need for more comprehensive management. Clinicians should increase their awareness of the broad impact of psoriasis on patients’ lives and the importance of psychosocial factors, such as body image and social emotional support, in the course of the disease. It is worth noting that the psychological impact of psoriasis is not in proportion to the severity of the disease. To understand the relationship between psoriasis and depression, one must take into account the patient’s subjective distress and the role of general societal pressure to achieve an ideal appearance, as well as the perceived importance of physical appearance in gaining societal worth and acceptance.
The authors thank all Polish psoriasis associations, particularly the Polish Association of Psoriasis Patients in Bydgoszcz, and the “Yes, I have psoriasis” Foundation in Lublin, Poland.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize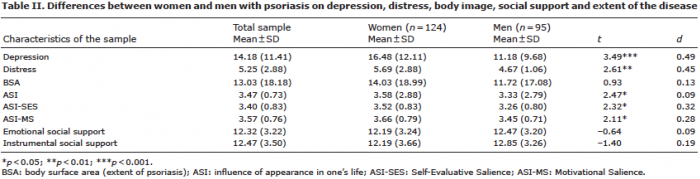 Click to show fullsize
Click to show fullsize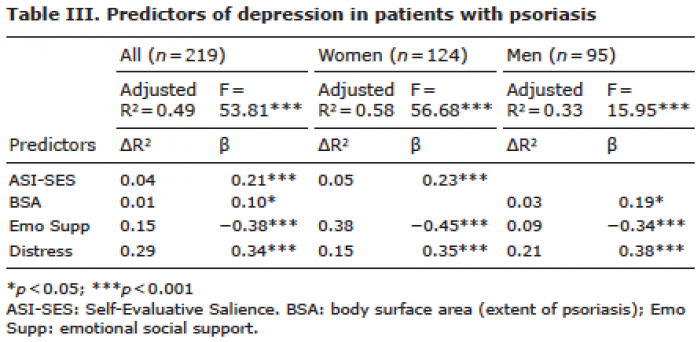 Click to show fullsize
Click to show fullsize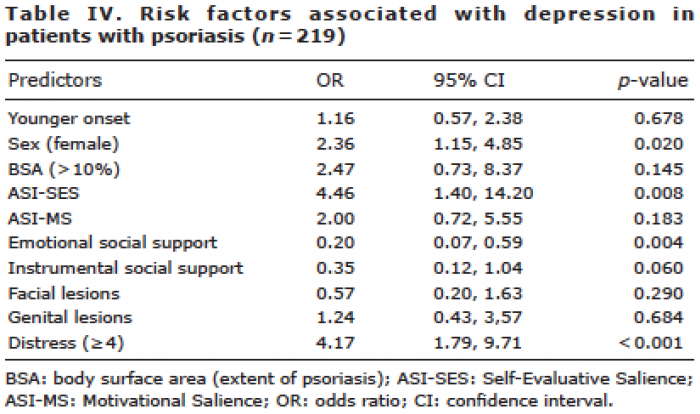 Click to show fullsize
Click to show fullsize