


Departments of Dermatology, Chonnam National University Medical School, 42 Jebong-ro, Dong-gu, Gwangju, 61469, South Korea. *E mail: yhwon@chonnam.ac.kr
Accepted Jun 1, 2016; Epub ahead of print Jun 15, 2016
Papulonecrotic tuberculid (PNT) is today rarely seen in effluent countries, but before the era of chemotherapy this was a rather common cutaneous manifestation of systemic tuberculosis. We present herein an unusual case of PNT in a child.
A 13-year-old girl from Korea presented with a 1-month history of asymptomatic papules and pustules on the extremities. The patient had a history of Bacillus Calmette-Guérin (BCG) vaccination. Three weeks previously she had visited a paediatrician for evaluation of a fever. At that time a chest radiography appeared normal, but a Mantoux test was strongly reactive (22-mm induration) and computed tomography showed multiple necrotic mesenteric lymph nodes. A QuantiFERON-Tuberculosis Gold In-Tube test (Cellestis Inc., Valencia, USA) was also positive. Recently, these interferon-γ release assays provide a fast and reliable diagnoses of cutaneous as well as systemic tuberculosis with high specificity and sensitivity (1). She was diagnosed with tuberculous lymphadenitis and treated with anti-tuberculous medication (rifampicin, isoniazid, pyrazinamide, and ethambutol). Subsequent physical examination in our department revealed multiple erythematous papules and pustules, 1–3 mm in diameter, not only on the extensor surfaces of her extremities and hands, but also on her palms (Fig. 1a–c). Several crater-like ulcers covered with crusts were observed on her left upper arm (Fig. 1d). Laboratory investigations for full blood count, renal, and liver function tests were normal, although the erythrocyte sedimentation rate was 108 mm/h (normal range 0~20 mm/h). Histopathological analysis of skin biopsies from the palm and forearm showed dense granulomatous cell infiltration with necrosis (Fig. 2). Mycobacterium tuberculosis was not identified on Ziehl-Neelsen staining of the skin specimen. Based on the clinical features, Mantoux test, and histopathological findings, a diagnosis of PNT associated with mesenteric tuberculous lymphadenopathy was established. The patient continued on anti-tuberculous medication for 6 months. Soon after treatment, remarkable clinical improvement was observed.
Fig. 1. Clinical features of the patient. (a) Multiple erythematous papules and pustules 1–3-mm in diameter on the left palm, (b) on the extensor surfaces of the right hand, and (c) on the left leg. (d) Several crater-like ulcers covered with crusts on the extensor aspect of the left upper arm.
Fig. 2. Histopathological analysis of skin biopsy (a, b) from the palm and (c, d) the forearm, showing dense granulomatous cell infiltration with necrosis. Haematoxylin and eosin (a, c) ×40; (b, d) ×100. The arrows direct a wedge-shaped area of necrosis forms, with its broad base toward the epidermis.
PNT is characterized by dusky red papules with a central depression, distributed symmetrically over the extensor aspects of the extremities, buttocks and lower trunk (2). The lesions may develop necrosis in the centre, leaving pitted scars. The disease is considered an id reaction to a particular tuberculous antigen and living organisms, mainly M. tuberculosis. The association of extracutaneous tuberculosis has been noted in approximately 40–75% of adult patients with PNT (2, 3). The cervical lymph node (19%) was the most common primary site, followed by the lungs (12%), bones (4%) and genitourinary tract (3%) (4). Jordaan et al. (3) showed that associated tuberculosis appears to be more prevalent in children. In contrast to adults, pulmonary tuberculosis was mostly reported. To date, 2 cases of mesenteric tuberculous adenopathy associated with PNT have been reported, with only one involving a child (2, 5). As far as we know, no case of PNT presenting papules and pustules on the palms has been reported previously. Histopathological results were consistent with PNT (see Fig. 2 a, b).
Clinically, PNT should be differentiated from pityriasis lichenoides et varioliformis acuta (PLEVA), papulopustular syphilid, perforating collagenosis, and perforating granuloma annulare (2). In addition, histo-logical differential diagnoses of PTN include PLEVA, inflammatory palisading granulomas, necrotizing vasculitis and Churg-Strauss granuloma (2). In summary, we describe here a rare case of PNT involving the palm, secondary to mesenteric tuberculous lymphadenopathy in a child. Physicians should recognize that papules and pustules may also involve the palms in PNT. In addition, subsequent evaluation of extracutaneous tuberculosis should include not only the lungs or cervical lymph nodes, but also the mesenteric lymph nodes.


 Click to show fullsize
Click to show fullsize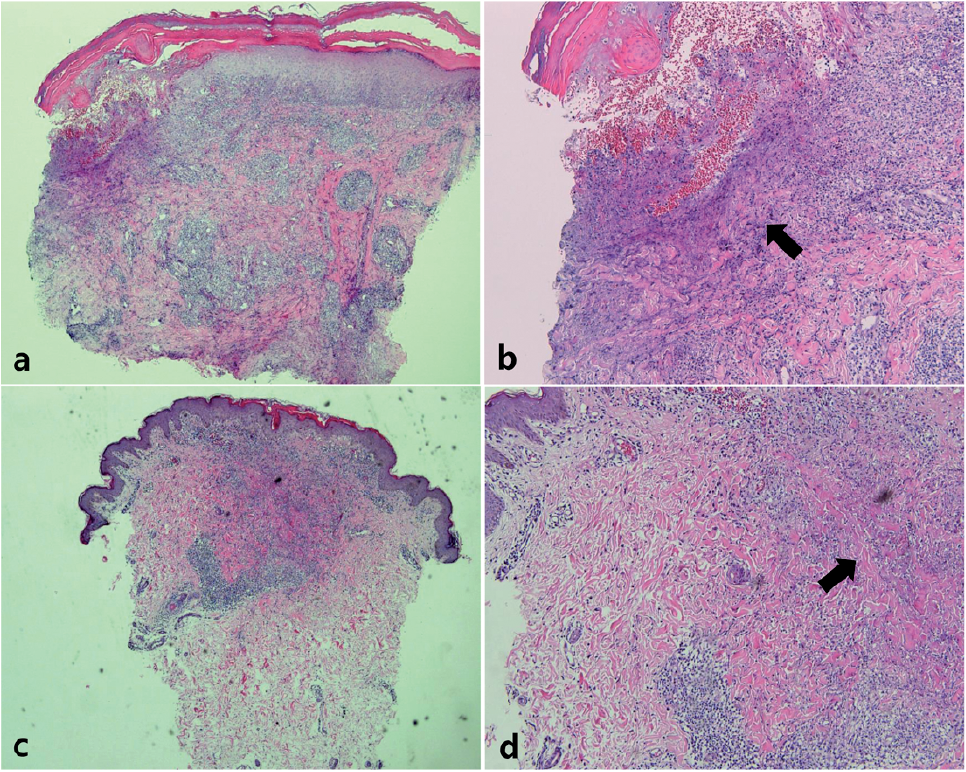 Click to show fullsize
Click to show fullsize