


1Psoriasis-Center, Department of Dermatology, and 2Section of Rheumatology, Comprehensive Center for Inflammation Medicine, University Medical Center Schleswig-Holstein, Campus Kiel, Schittenhelmstr. 7, DE-24105 Kiel, Germany. E-mail: umrowietz@dermatology.uni-kiel.de
Accepted Jun 15, 2016; Epub ahead of print Jun 28, 2016
Alopecia areata (AA) is an autoimmune condition resulting in the loss of scalp hair, or in alopecia areata universalis of the entire body hair, including the eyebrows and eyelashes. There is no approved treatment. Recommended guideline drugs are ineffective in inducing lasting hair regrowth.
We describe here a young woman who developed AA universalis at the age of 18 years, with complete loss of scalp hair, eyebrows, eyelashes and body hair. At the time of first occurrence of alopecia she had also had thyroid dysfunction and plaque psoriasis since the age of 17 years. Treatment of AA included topical steroids and systemic steroid pulse therapy with no effect on hair growth. When she first presented at our department AA had been present for 2 years and she reported swelling and pain in the second digit of her right hand, being unable to bend the finger.
Physical examination revealed complete hair loss, but dermoscopic evaluation confirmed the presence of hair follicles. She presented with typical psoriasis plaques on the scalp, arms, genital area and trunk, with additional involvement of all fingernails and toenails with an initial Psoriasis Area and Severity Index (PASI) of 7.7.
There was no family history of AA, but her mother had psoriasis. The patient reported a need for psychological intervention because of her AA. She was on a stable medication of 75 ?g L-thyroxin per day.
Rheumatologist consultation and magnetic resonance imaging (MRI) confirmed the diagnosis of acute dactylitis as a first manifestation of psoriatic arthritis. Laboratory findings showed no abnormalities.
In searching for a treatment that could be beneficial for AA, plaque psoriasis and psoriatic arthritis, we were reminded of a case report by Craiglow & King (1) describing successful therapy of AA in a patient with plaque psoriasis, with the janus-kinase (JAK)-inhibitor tofacitinib, which is registered in some countries for rheumatoid arthritis.
Since tofacitinib is not registered in Germany we applied for reimbursement from the patient’s healthcare insurance and achieved approval limited to a period of 6 months.
Treatment was started at a dose of 15 mg/day. After 4 weeks significant hair regrowth was seen on the scalp, in particular in the areas with psoriasis lesions. Pain and swelling of dactylitis was completely gone and the patient could bend her finger again. With ongoing tofacitinib therapy hair continued to grow on all body sites, except for the eyebrows and eyelashes. Interestingly, there was no effect of tofacitinib on psoriasis lesions that needed additional topical therapy with various agents, including mometasone furoate and the fixed combination of betamethasone and calcipotriol. After 6 weeks of therapy the patient developed a herpes zoster infection (C6 right side), which was treated with a course of oral brivudine with complete resolution after 2 weeks. Because of the continuous significant hair growth and the resolution of psoriatic arthritis symptoms the dose of tofacitinib was reduced to 10 mg/day. Tolerability was excellent except for mild chronic obstipation since the start of treatment with tofacitinib.
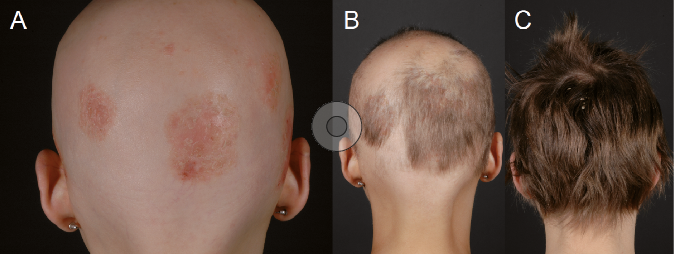
After 6 months the patient’s scalp hair was approximately 5 cm long with no remaining patches of AA (Fig. 1). Upon request we were granted approval from the patient’s healthcare insurance to continue therapy for another year.
Fig. 1. (A) Scalp hair loss and psoriasis lesions at first presentation. (B) New hair growth with preference for lesional psoriasis skin 3 months after initiation of tofacitinib, 15 mg/day. (C) After 7 months, at the current dose of 10 mg/day.
The patient has now been treated continuously for 9 months with 10 mg/day tofacitinib, with continuing hair growth, complete resolution of dactylitis, and no other symptoms of psoriatic arthritis, but with the development of new psoriasis lesions particularly on the scalp that are refractory to conventional topical therapy. With the addition of low dose oral fumaric acid ester therapy psoriasis lesions are now resolved.
AA universalis is an inflammatory disease of unknown aetiology and unpredictable course that leads to a significant impairment of health-related quality of life and is associated with a high burden of disease (2). Since the pathogenesis of the disease is unknown, no rational treatment can be applied. Topical steroids and/or systemic steroids are recommended after first disease occurrence (3). Other options are the induction of contact allergy by application of contact sensitizers, such as diphencyprone or anthralin, to induce an irritant reaction.
In 2014 Xing et al. (4) described the dependency of a mouse model of AA on the janus kinase (JAK) system and presented evidence that patients with AA treated with the oral JAK1 and JAK2 inhibitor ruxolitinib showed near-complete hair regrowth within 5 months of therapy.
Supporting the first case report (1), Jabbari et al. (5), recently published a case of AA controlled by the JAK1/2 inhibitor baricitinib.
In the current report we show that, in refractory AA universalis, complete hair growth was achieved soon after initiation of tofacitinib therapy. In addition, there was a rapid and complete response of psoriatic arthritis/dactylitis; however, plaque psoriasis not only remained unchanged but worsened under continued tofacitinib therapy. Apart from the episode of uncomplicated herpes zoster and mild chronic obstipation there was no safety issue and the drug was well tolerated.
There is debate as to whether JAK inhibitors that can be used in man so far are specific for JAK isoforms such as JAK1, JAK2 or JAK3 or whether they can be regarded as pan-JAK inhibitors. Tofacitinib is thought primarily to inhibit JAK 1 and 3 and therefore seems suitable to treat AA. With regard to the dose it was shown that, in the reported case, 15 mg/day initially and thereafter 10 mg/day was sufficient to control hair growth and psoriatic arthritis. The interesting observation that plaque psoriasis shows no treatment benefit may be due to an insufficient dose, as in clinical trials of tofacitinib in plaque psoriasis up to 20 mg/day were required to induce remission of lesions (6, 7); however, due to healthcare restrictions it was not possible to give this dose in this patient. In psoriatic arthritis tofacitinib, 5 mg twice daily, showed an American College of Rheumatology 50 (ACR50) response in 75% of patients and a PASI 75 in 62.8% (8). This data suggests a higher efficacy in psoriatic arthritis, which is in line with our observation here.
From a clinical perspective it was interesting to see the first and very rapid hair growth, nearly exclusively on the area of pre-existing psoriasis plaques, on the patient’s scalp.
Clinical trials with ruxolitinib and tofacitinib for AA are ongoing and, in the future, JAK-inhibitors may become a first-line therapy for an otherwise refractory disease.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize