


1Center for Chronic Pruritus, Department of Dermatology, 2Institute of Medical Informatics, University Hospital Mu?nster, Münster, and ³Institute for Clinical Diabetology, German Diabetes Center, Heinrich Heine University, Düsseldorf, Germany
Patients with chronic pruritus may develop scratch-induced lesions with elevated borders and central necrosis. This so-called umbilicated type of prurigo (UP) is rare and is assumed to develop preferentially in the context of metabolic diseases. The aim of this study was to characterize UP in its clinical and histological dimension. Demographic and clinical data were collected from 23 patients with UP. Intensive light microscopical analysis of biopsied lesions was performed. Statistical comparison with previous results for prurigo nodularis (PN) showed that UP is clearly a subtype of PN. In addition, clinical and microscopic features of epidermal perforation identical to those in acquired reactive perforating dermatosis (ARPD) were observed. Hence, we suggest that ARPD is identical to UP and is therefore a subtype of PN. We assume that reduced wound healing capacities due to underlying systemic disorders, particularly diabetes mellitus and uraemia, underlie the pathomechanism of development of umbilicated skin lesions with a perforating aspect.
Key words: Kyrle; prurigo; pruritus; itch; perforating dermatosis.
Accepted Jun 15, 2016; Epub ahead of print Jun 28, 2016
Acta Derm Venereol 2017; 97: XX–XX.
Corr: Roxane-Isabelle Kestner, Department of Dermatology, University Hospital Mu?nster, Von-Esmarch-Str. 58, DE-48149 Mu?nster, Germany. E-mail: roxane-isabelle.kestner@kgu.de
A
lthough many attempts have been made to define prurigo, this term is still used inconsistently for a heterogeneous group of skin conditions (1). A new classification, focused on clinical criteria, has been established recently by Schedel et al. (2), which clearly differentiates between primary skin diseases (e.g. actinic prurigo) and secondary reaction patterns, such as prurigo nodularis (PN). Following this classification, PN must be understood as a reactive disease due to permanent scratching. According to the suggested definition, PN is a skin disorder characterized by intensely pruritic, hyperkeratotic and indurated papules, nodules or plaques. Lesions tend to exhibit superficial erosion, while deep excoriation is a possible, but rare, feature. Interlesional skin is frequently lichenified. Association with chronic itch is obligatory, as is the preferential occurrence of lesions on areas easily reachable for scratching. Affected sites are mostly on the extensor surfaces of the extremities and the trunk, especially the neck and lower back. On the back, lesion-free regions may be observed in areas where it is difficult for the patient to reach to scratch (“butterfly sign”). To date, the pathogenesis of PN is not completely understood. It is assumed that a complex neuroimmunological interaction of mast cells and eosinophilic granulocytes releasing neurotrophins (3, 4) and pruritogenic cytokines, such as IL-31 (5), leads to neuronal stimulation and growth (6).
In addition to the classical papular and nodular types of PN, which may represent different stages of the same phenomenon, 2 special forms are mentioned in Schedel’s work (2): (i) ulcerated prurigo, which is associated with extensive, deep scratching, and (ii) umbilicated lesions. This latter type is little-known in today’s clinical practice and is usually classified as a perforating dermatosis. According to Schedel et al. (2) umbilicated prurigo lesions are specifically characterized by an elevated epidermal border surrounding a central area of eschar-like necrosis, which led to their naming. A strong connection between umbilicated prurigo and systemic internal diseases was assumed (2).
Similar skin alterations have been described, first in 1916 by Josef Kyrle (7), who paid particular attention to the histological aspect of cup-shaped epidermal impressions surrounded by hyperplastic epidermis. As those impressions filled with cellular debris spanned through all epidermal layers, and their ground showed focal absence of the basal membrane, he introduced the concept of “epidermal perforation”. Kyrle’s disease became the leading disorder of a new group of diseases: the perforating dermatoses.
We hypothesized that umbilicated prurigo is part of the prurigo spectrum, and of the perforating skin disorders. To investigate this and to embed umbilicated prurigo (UP) into those groups, we characterized UP clinically, histologically and aetiologically by collection of demographic data, detailed histological analysis and statistical comparison with criteria of PN. Furthermore, an aim of this study was to show that focussing on clinical patterns might help the move away from confusing and redundant terms in favour of clearly distinguishable conditions.
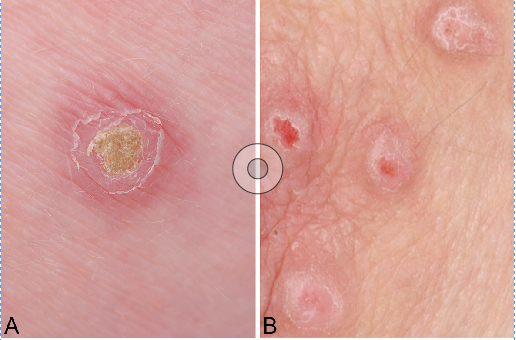
Twenty-three patients with chronic pruritus were included in this retrospective study. All were patients of the Center for Pruritus of the University Hospital Münster and underwent diagnostics for the underlying origin of chronic pruritus. Skin biopsies for routine purposes were obtained during a period from January 2008 to January 2013. Only persons who clearly fulfilled the clinical criteria of UP were included in this study, defined by the presence of multiple exulcerated lesions with eschar-like necrosis in the centre scattered over the body. An important criterion was that the lesions were surrounded by a raised, erythematous rim. Photographic documentation exists in 9 of 23 cases (Fig. 1). Demographic parameters, including age and sex, as well as pruritus parameters, such as mean and maximum intensity, duration, localization at the beginning and over the whole period of the study, response to physical stimuli (touching, local pressure, scratching, coldness) and accompanying sensations (stinging, tingling, burning) were collected from patient files based on patient interviews, questionnaires and physical examination. Medical history data were collected regarding comorbidities, current medication and surgery until the investigation date. Approval of a local ethics committee for retrospective data analysis was secured (No. 2007-413-f-S, 2008-235-f-S). The study was registered in the German registry for clinical trials (DRKS00009779).
Fig. 1. Clinical findings. (A) umbilicated prurigo and (B) classical prurigo nodularis. Comparison of umbilicated prurigo lesions on the upper leg and prurigo nodularis nodules on an elbow. (A) The special shape of the lesions is crucial for diagnosis of umbilicated prurigo: a central brownish plug is surrounded by an elevated erythematous rim. (B) Two of the nodules of classical prurigo nodularis show superficial excoriations, while necrosis is lacking.
Most biopsies (n = 17) were taken for diagnostic purposes from the rim of the lesions. Six specimens also show the centre. The appearance and severity of clinical features did not differ between the 2 groups. Three-step sections of each specimen were stained with haematoxylin-eosin and Weigert’s elastic stain and analysed by 2 independent histologists (DM, RK). For visualization of collagen fibres polarization was used. Criteria included all parameters previously described by Weigelt et al. in 2010 to characterize the histological appearance of PN (8) and additional features of acquired reactive perforating dermatosis. Special attention was paid, if shown in our specimens, to epidermal perforation of collagen and the composition of the covering debris.
Statistical comparison with the histological features of classical PN, described by Weigelt et al. 2009 (8), was used to embed this rare subtype into the PN spectrum. Data were collected and analysed using SPSS Statistics Version 22 for Microsoft Windows. Description of our patients’ demographic and medical data was done using frequency tables, and comparison with histological criteria of PN by using cross tables. Results with p < 0.05 were accepted as significant.
A total of 23 patients (14 females, 9 males; age range: 38–93 years; mean ± SD: 70.5 ± 12.2 years) with clear clinical diagnosis of umbilicated prurigo (Fig. 1) as defined by the presence of multiple exulcerated lesions with an impressed, eschar-like necrotic centre, were included in this study. These lesions occurred in different age and at different body parts. They were always surrounded by an elevated epidermal rim and could be clearly distinguished from common PN nodules (Fig. 1). To a lesser, and more variable, extent the patients also showed classical papular, nodular, and plaque types of PN, although the majority of lesions were still of the umbilicated type. All patients had chronic pruritus. Mean ± SD visual analogue scale pruritus intensity score was 6.2 ± 1.8. Mean ± SD maximum intensity was 8.7 ± 1.5. Accompanying sensations, such as burning, stinging or tingling, were described (n = 15; 65.2%). Appearance of umbilicated prurigo lesions was strongly connected with the occurrence of pruritus in the affected body parts. Only 2 patients showed generalized pruritus at the beginning of the study, while 19 (82.6%) developed generalized itch over the time. If localized at the beginning of the study, the trunk was affected in 52.4% of cases. In 33.3% of patients, the disorder started on the lower extremities. Most patients experienced relief of pruritus by scratching (n = 14; 63.6%) or cold (n = 11; 52.4%), and worsening by touching and pressure (n = 12). A summary of pruritus parameters is shown in Table I.
Table I. Demographic and clinical data including pruritus parameters, in 23 patients
The most important aetiology of pruritus was diabetes mellitus (69.7%), followed by chronic kidney disease (n = 9; 39.1%). Other not-pruritus-related comorbidities (Table I) comprised endocrinological (82.6%) and cardiac (73.9%) diseases with the predominant presence of arterial hypertension (n = 12; 52.1%), gastrointestinal conditions, such as liver and gall bladder impairment, neurological features, such as epilepsy or apoplexy, and orthopaedic impairment, especially disc protrusion/herniation. Disorders of the genitourinary system, the eyes and ears and the patients’ mental state were comparatively rare. Two patients did not report any relevant past medical history.
In 22 of 23 cases epidermal hyperplasia was seen, of which 16 (69.6%) could be diagnosed as irregular and 5 (21.7%) as pseudoepitheliomatous. One specimen clearly showed a plump hyperplastic epithelium devoid of rete ridges, one showed no epithelial hyperplasia. Focal parakeratosis was a common feature (n = 16; 69.6%) in addition to orthohyperkeratosis, which was found in a lamellar aspect in 12 cases (52.2%) and in a compact aspect in 8 cases (34.8%). In 3 biopsies (13.0%) ortho-hyperkeratosis was absent. The epidermis presented haemorrhagic inclusions (n = 10; 43.5%), defect of a haemorrhagic corneum (n = 4; 17.4%), erosions (n = 2; 8.7%) and deep excoriations (n = 7; 30.4%). Hypergranulosis appeared in 82.6% (n = 19). Keratinocytes occasionally happened to be hyperpigmented (n = 9; 39.1%) or multinucleated (n = 11; 47.8%). We found extravasal erythrocytes in 18 biopsies (78.3%). Fibrosis of the dermis was strikingly prominent (n = 22; 95.7%), and was characterized, for example, by the occurrence of thickened collagen fibres (n = 21; 91.3% in the papillary dermis and n = 23; 100% in the reticular dermis), increased number of fibroblasts (n = 22; 95.7% in the papillary dermis and n = 19; 82.6% in the reticular dermis), and loss of elastic fibres. Melanophages could be found in 7 cases, 30.4%. Inflammatory infiltrate was an important feature in all specimens. It always appeared in perivascular sites, in 87.0% (n = 20) it was also present superficially and in 69.6% (n = 16) it was present in deep parts of the dermis. Interstitial infiltration was rarely seen (n = 6; 26.1%). The infiltrate was dominated by lymphocytes (n = 23; 100.0%) and macrophages (n = 22; 95.7%). In addition, granulocytes were seen frequently (eosinophils in 15 cases, 65.2% and neutrophils in 13 cases, 56.5%). Six specimens showed a cup-shaped depression filled with cellular debris, serum, blood, and inflammatory cells accompanied by bacteria. In addition, vertical collagen fibres were always observed within the debris (Figs 2 and 3). Collagenous material, although fading in HE disability, could be proven inside the plug in 6 cases by polarization microscopy. Notably, granulation tissue was almost completely absent under the skin defect.
Fig. 2. Histological findings in umbilicated prurigo. Epidermal depression filled with basophilic debris and inflammatory cells. The raised epidermal edge is hyperplastic and shows parakeratosis. At the lesion’s ground the epidermal layer is thin and occasionally disrupted. Vertical collagen fibres pass through the gaps into the plug. A small vessel surrounded by perivascular infiltrate is depicted as well as superficial fibrosis and infiltra-tion (Polarization light, × 400).
Fig. 3. Umbilicated prurigo lesion in polarization microscopy. At the basis of the epidermal depression vertically arranged collagen fibres can be seen to pass through into the overlaying debris. Expression of collagenous material is also proven in the upper parts of the necrotic plug (Polarization light, × 400).
In comparison with the findings previously described in PN (8), our sample confirmed the main criteria of PN, which often occurred even in a significantly higher percentage or grade than reported previously (8). Both groups showed mostly irregular epidermal hyperplasia, orthohyperkeratosis and hypergranulosis. Interestingly orthohyperkeratosis was more often lamellar in our specimens (n = 12; 52.2%; p < 0.001) and parakeratosis occurred more frequently (n = 16; 69.6%; p = 0.006). As expected, epidermal hemorrhagic inclusions and epidermal defect, as well as extravasal erythrocytes, were more prominent in our biopsies (p < 0.001).
While dermal fibrosis is an important finding of PN (n = 71; 52.2%), it is even more prominent in the umbilicated type (n = 19; 82.6%) and tends to involve the reticular dermis (p < 0.001) in particular.
The only main feature of PN that is under-represented in our specimens is the density of inflammatory infiltrate, which is moderately present in Weigelt’s data (44.1%) and low in the biopsies presented in this study (n = 19; 82.6%). However, the infiltrate’s composition, with dominance of lymphocytes and macrophages, did not differ between the 2 groups. All histological data are summarized in Table II.
Table II. Histological findings in umbilicated and classical prurigo nodularis
The prurigo spectrum, as well as that of perforating dermatoses, has undergone continuous reclassification and enlargement, resulting in a loss of focus on which phenomena belong together. Nowadays, chronic mechanical skin traumatization, e.g. due to permanent scratching, is accepted as the pathogenetic basis of members of both groups of conditions (2, 9). UP, a rare phenomenon presented in this study, shows characteristics of classical PN as well as of perforating disorders, and might even be identical to acquired reactive perforating dermatosis (ARPD).
This study showed that all histological criteria of classical PN are fulfilled in UP, which must therefore be considered as a subtype of scratch-associated prurigo, as already outlined by Schedel et al. (2). Weigelt et al. (8) defined PN histologically in 2010. The pathognomonic constellation of features illustrated in their work includes thick, compact hyperkeratosis (part of the “hairy palm sign”), irregular and pseudoepitheliomatous hyperplasia accompanied by focal parakeratotic sites and hypergranulosis, fibrosis of the papillary and reticular dermis and a mainly perivascular and superficial inflammatory infiltrate dominated by lymphocytes and macrophages. Remarkably, most of our specimens not only showed all those criteria, but also tended to express them in a significantly higher number or grade than in the previously investigated PN collective (Table II). While the bases of the pathomechanism of both nodular and umbilicated prurigo might be the same, UP differs by underlying metabolic imbalances. Together with the observation that almost all of our patients with UP were either diabetic or nephrogenic or both, we hypothesize that UP evolves in the context of a metabolic disturbance. Amongst other systemic diseases diabetes and chronic kidney disease are known to predispose to severe pruritus (10, 11). Remarkably they are also strongly associated with impaired healing of dermal wounds. Advanced glycation end-products (AGEs) have been shown to disturb cell-collagen interactions, remodelling of the extracellular matrix and epidermal cell recruitment, which causes delay to wound closure (12). AGEs may further hamper wound healing by induction of diabetic macro- and micro-angiopathy (13). Skin collagen AGEs are strongly associated with the future development of diabetic retinopathy, nephropathy and neuropathy over up to 17 years in subjects with type 1 diabetes (14). It has been shown recently that subjects diagnosed with type 2 diabetes show a pronounced reduction in epidermal Langerhans cells density, which could be another predisposing factor for cutaneous infection, impaired wound healing and foot ulceration (15). In addition, uraemia is characterized by the accumulation of AGEs as well as of advanced lipoxidation end products (ALEs) independently of coexisting diabetes mellitus (16). Chronic kidney disease was shown to be accompanied by decreased cell proliferation and angiogenesis, as well as reduced granulation tissue and re-epithelialization of wounds (17). Thus, it seems likely that superficial erosions could easily emerge into excoriated and partly necrotic lesions in diabetic and nephrogenic patients with chronic pruritus.
In addition, the dermal reaction appears to be altered in UP. Although papillary and reticular fibrosis is one of the main features of PN in general, the umbilicated type is characterized by a pronounced fibrotic reaction, especially in deeper dermal parts. Fibrosis and infiltration seem to follow the ulceration vertically. It is notable that the density of inflammatory cells is lower in the UP collective and the occurrence of granulation tissue is clearly reduced in comparison with cases of classical PN. This is interpreted as the key feature in the development of UP lesions. While injuries of the skin in classical PN are restricted to occasional superficial excoriations, umbilicated lesions show a deep epidermal impression incidentally with destruction of the basal membrane at the lesions’ ground. As a consequence, vertically arranged collagen fibres can pass through the resulting gaps into the intraepidermal plug, as is known for perforating dermatoses (18) (Fig. 3).
The ARPD comprise 4 main entities: Kyrle’s disease, perforating folliculitis, elastosis perforans serpiginosa and reactive perforating dermatosis, which were originally distinguished by the special composition of the material extruded through an epidermal defect (18). Over the past 100 years multiple subtypes and terms had been added to this group, classifications had been altered and definitions became unclear. Several studies have shown that both collagen and elastin, as well as components of the extracellular matrix, are discharged in lesions of all subtypes of perforating dermatoses (19–23). Interestingly, our analysis of the plugs in umbilicated prurigo showed the same composition (Table II). Gambichler et al. (24) suggest an interplay of microtraumatization, altered wound-healing capacities and tissue hypoxia due to diabetes- and uraemia-associated microangiopathy and oxidative stress as the basic pathogenetic mechanism of ARPD. Moreover, typical lesions are preferentially located on trauma-prone areas (9) and even showed experimental inducibility (25).
The patients presenting with UP in our study fit perfectly to the description and picture of ARPD: they have generalized to localized typical lesions with a particular preference for the trunk and extremities. Intact prurigo nodules, including papular, nodular and plaque type, occur in addition to ulcerated centrally necrotic lesions surrounded by a raised edge. This clinical aspect was crucial for the diagnosis of UP and inclusion in this study. Correlation with mean to severe pruritus and permanent scratching were omnipresent in this collective. The high incidence of concomitant sensations, such as burning and tingling, is interpreted as a strong hint for neuropathic mechanisms typical for diabetogenic or nephrogenic pruritus (26).
This study is limited by the fact that the analysed biopsies were acquired not in a prospective setting, but from diagnostic routine in our itch clinic. Therefore most specimens were taken from the lesions’ rim, which is important for analysis of features of classical PN. The low number of biopsies from only one centre may not be representative. However, exemplary for the whole collective, 6 biopsies show the complete lesion. Beyond that, the biopsies showing the centre of the lesions or the rim only do not differ clinically or statistically, thus the same histological image of the central plug can also be expected in the other specimens.
In conclusion, consistent with explanatory approaches to ARPD and PN, we assume that the underlying pathomechanism of UP is based on a specific imbalance of reparative processes of the metabolically altered extracellular matrix and oxygen supply in microangiopathic dermis associated with permanent traumatization. What we describe in this study is a special disorder that can be undoubtedly subgrouped into the prurigo spectrum, but at the same time shows all criteria of ARPD. Hence, we suggest that ARPD is identical to umbilicated prurigo, and is therefore a subtype of PN, which requires a search for metabolic diseases followed by causative therapy.


 Click to show fullsize
Click to show fullsize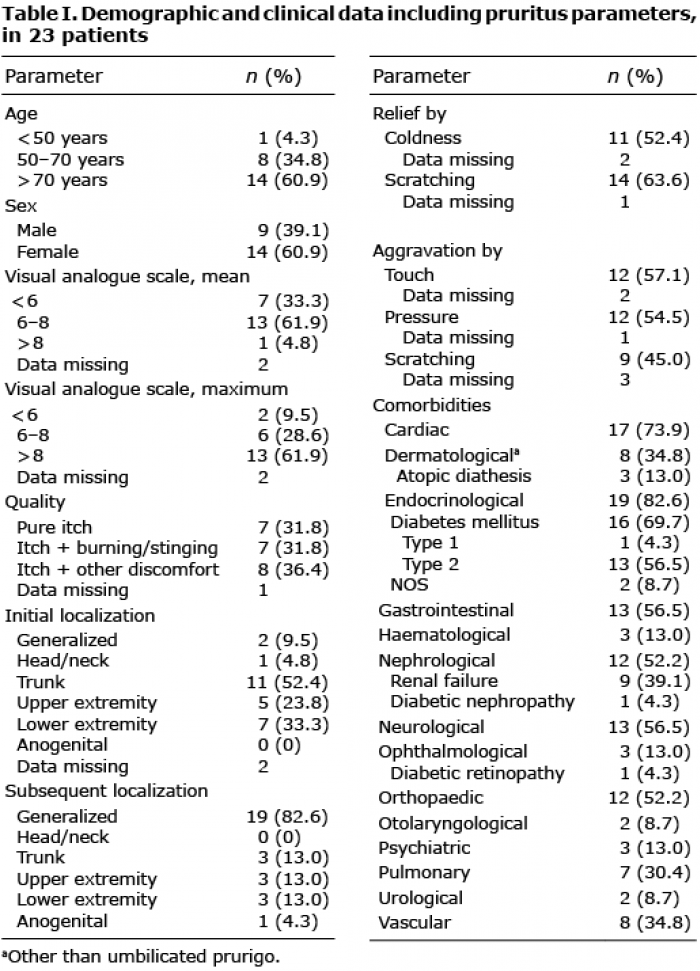 Click to show fullsize
Click to show fullsize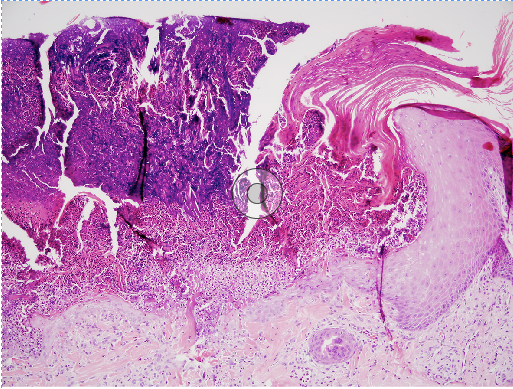 Click to show fullsize
Click to show fullsize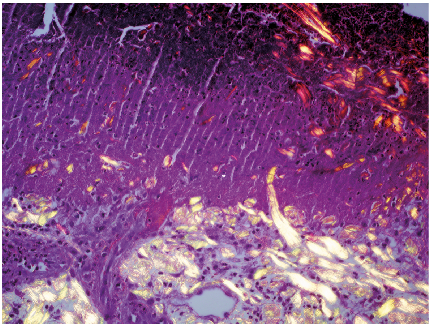 Click to show fullsize
Click to show fullsize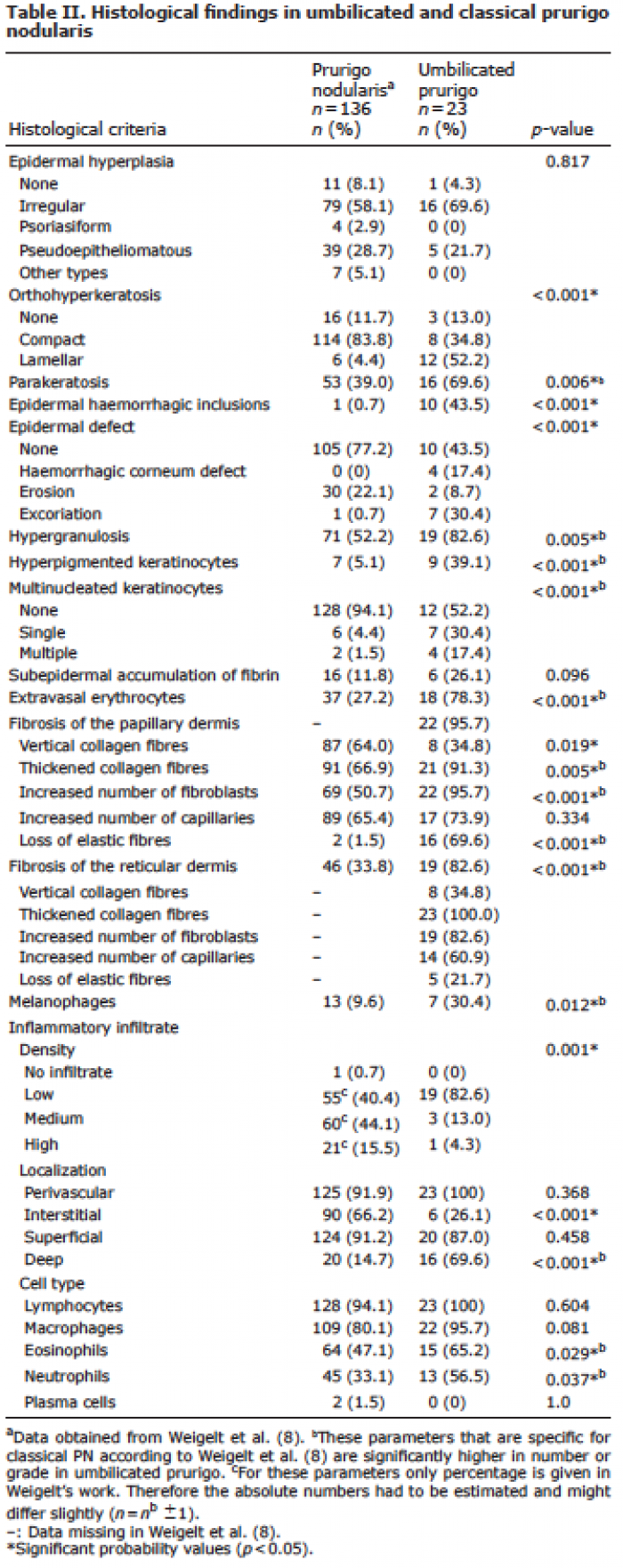 Click to show fullsize
Click to show fullsize