


Division of Dermatology, Department of Medicine of Sensory and Motor Organs, Faculty of Medicine, Tottori University, 36 Nishi-cho, Yonago 683-8504, Japan. E-mail: r-ttm@med.tottori-u.ac.jp
Accepted Jun 15, 2016; Epub ahead of print Jun 28, 2016
Imiquimod, a ligand for Toll-like receptor (TLR) 7, can induce psoriasis in focal and generalized patterns (1, 2). Previous studies have shown that symptoms usually improve with topical application of calcipotriol or steroids and/or ultraviolet B treatment (1, 2). We describe here a case of imiquimod-induced psoriatic erythroderma treated with infliximab in a patient with no history of psoriasis.
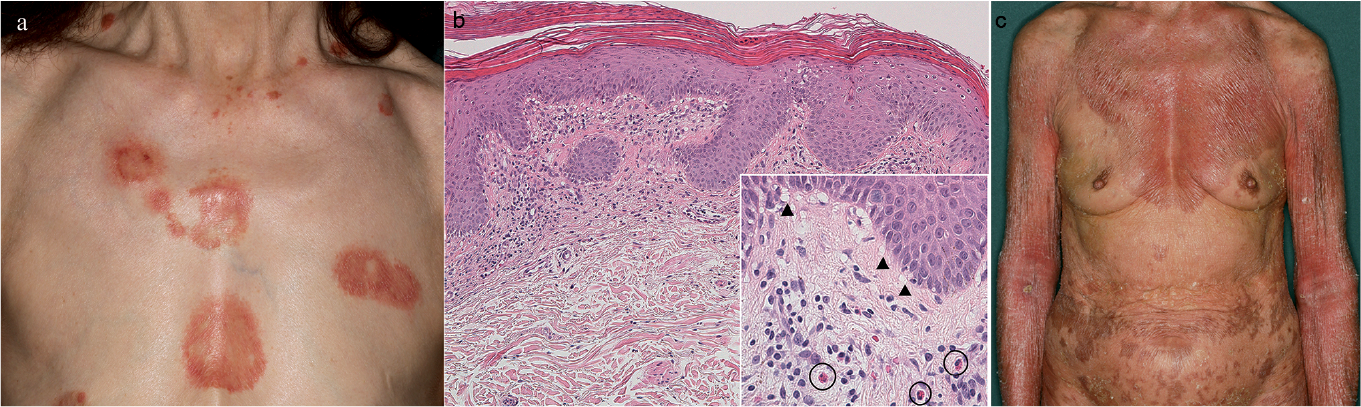
A 78-year-old woman presented with a 1-year history of scaly erythema in her right cheek. A diagnosis of actinic keratosis was made by biopsy showing proliferation of atypical keratinocytes in the epidermal basal layer. After topical application of 5% imiquimod cream, 250 mg/day every other day for 6 weeks, the lesion disappeared. One month later, scaly erythemas developed on her glabella and back and then extended to her trunk and extremities. Physical examination revealed isolated erythemas accompanied by whitish scales without exudative change, principally involving intertriginous areas (Fig. 1a). Results of laboratory investigations (full blood count, electrolytes, liver function tests, renal function and soluble interleukin-2 receptor) were unremarkable. Whole-body computed tomography scanning did not reveal any malignancy. She was not on any regular medication and had no personal and family medical histories of psoriasis and dermatitis, including atopic dermatitis and seborrhoeic dermatitis. No fungus was found in the scales by direct microscopy. At first, we suspected psoriasis vulgaris, pustular psoriasis or auto-sensitization dermatitis. A skin biopsy specimen from the erythema on the patient’s back showed early signs of psoriasis: focal parakeratosis, mild acanthosis with elongated rete ridges and dilated vessels in the papillary dermis (Fig. 1b). In addition, lichenoid reaction was observed: vacuolar degeneration of the basal layer and dense infiltration of lymphocytes and eosinophils in the upper dermis. We began topical application of clobetasol propionate, but the response was poor. Based on the clinical and histopathological findings, a diagnosis of imiquimod-induced psoriasis was made. Since the patient’s eruptions worsened, she was hospitalized. Although we treated her with application of calcipotriol and oral etretinate, 30 mg/day, in combination with psoralen plus ultraviolet A (PUVA)-bath treatment (total 6.1 J/cm2), the response was poor, resulting in erythroderma (Fig. 1c, Fig. S1a). A second skin biopsy from the buttock showed features of psoriasis: confluent parakeratosis, hypogranulosis and thinning of the epidermis on the papillary dermis (Fig. S1b). Vacuolar degeneration of the basal layer and perivascular infiltration of lymphocytes and eosinophils in the upper dermis were also observed. Finally, infliximab, 5 mg/kg (210 mg), was administered and the erythemas improved dramatically within several days. After administration 5 times at 8-week intervals, only inconsequential lesions remained on her face and lower extremities (Fig. S1a). Notably, as well as the dramatic improvement in eruptions, serum tumour necrosis factor (TNF)-α level decreased in response to administration of infliximab (from 10.1 pg/ml on the 3rd day to 0.9 pg/ml on the 44th day after initial injection of infliximab) (normal: 0.6–2.8 pg/ml).
Fig. 1. (a) Scaly erythema on the chest (10 weeks after the beginning of imiquimod application). (b) First skin biopsy from the back revealed lichenoid changes: basal vacuolar change (arrowheads) and infiltration of lymphocytes and eosinophils (circles) in the upper dermis as well as early psoriatic change (haematoxylin and eosin stain) (original magnification ×100, inset: ×200). (c) Psoriatic erythroderma (before treatment with infliximab). The identity of the patient has been protected.
Psoriasis is one of the most common immune-mediated chronic inflammatory skin disorders accompanied by erythematous scaly plaques (3). Psoriatic lesions are characterized by histopathological features, including acanthosis, confluent parakeratosis and dermal infiltration of immune cells (3). Several drugs have been reported to result in exacerbation of pre-existing psoriasis or initiation of psoriatic lesions that are termed “drug-induced psoriasis” (4, 5). Histopathologically, drug-induced psoriasis shows not only the typical features of psoriasis, but also a lichenoid pattern and dermal eosinophil infiltration (6, 7).
Imiquimod-induced psoriasis has sometimes been described in adult patients with a prior history of psoriasis (1, 8). Moreover, there have been a few reports in children (2). In most previous studies, the symptoms were resolved by only application of topical calcipotriol or topical steroids and/or ultraviolet B treatment (1, 2). There have been 2 reports of treatment with infliximab, a chimeric monoclonal antibody against TNF-α, in the course of imiquimod-induced psoriasis, because of a flare of the patient’s skin condition and complication of arthritis (8). However, the patients had pre-existing psoriasis, and new lesions developed at the site of imiquimod administration. In contrast, our patient had no previous history of psoriasis. The psoriatic lesions arose from regions away from the site of imiquimod application, resulting in psoriatic erythroderma.
Although the pathogenesis of imiquimod-induced psoriasis is unclear, several theories have been discussed (9–15). TLR 7-mediated secretion of interferon-α from plasmacytoid dendritic cells is involved in the primary mechanism, leading to activation of the adaptive immune system, specifically Th1 and Th17 cells (9). TNF-α was shown to play a significant role both in a mouse model and in humans (10–12); knockout mice lacking receptors to TNF and/or interferon showed protection against imiquimod and reduced levels of inflammatory cytokines (13). IκBζ has been identified as a key regulator in imiquimod-induced psoriatic inflammation in a mouse model (14).
In our patient, serum TNF-α level decreased in response to administration of infliximab, and the intract-able eruptions were improved. This fact corresponds to the suggestion that TNF-α plays a significant role in imiquimod-induced psoriasis.
It is important for clinicians to consider the possibility of imiquimod-induced psoriasis in cases of newly intractable erythemas after the application of this drug. A detailed drug history and histopathological examination are essential for accurate diagnosis. Even topical medicine, such as 5% imiquimod cream, can cause severe and persistent psoriasis requiring treatment with anti-TNF-α inhibitor drugs.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize