


1University of Rochester Medical Center, Department of Dermatology, Rochester, NY, USA, 2Allergy Section, Division of Immunology, Department of Internal Medicine, College of Medicine, University of Cincinnati, Cincinnati, OH, USA, and 3Department of Dermatology and Allergy, Charité – Universitätsmedizin Berlin, Berlin, Germany
Both spontaneous and inducible forms of chronic urticaria pose a significant economic burden and have an adverse effect on patients’ quality of life. The international guidelines and US practice parameters for the diagnosis and management of chronic urticaria both recommend performing a thorough patient history and physical examination, conducting limited routine laboratory testing, and taking a stepwise approach to treatment. These documents differ in several areas, such as the order of diagnostic procedures and the treatment for patients non-responsive to standard dose H1-antihistamines. Patients with chronic urticaria who visit a specialist have typically been treated with second-generation H1-antihistamines – the recommended first-line treatments. The advantages and disadvantages of each treatment option should be taken into consideration when selecting therapies beyond H1-antihistamines. Greater awareness of the international guidelines and US practice parameters will likely improve the quality of care for patients with chronic urticaria.
Key words: chronic spontaneous/idiopathic urticaria; physical urticaria; inducible urticaria; wheal; hives; guidelines.
Accepted Jun 15, 2016; Epub ahead of print Jun 28, 2016
Acta Derm Venereol 2017; 97: XX–XX
Corr: Lisa A. Beck, MD, University of Rochester Medical Center, School of Medicine and Dentistry, 601 Elmwood Ave, Box 697, Rochester, NY 14642, USA. E-mail: lisa_beck@urmc.rochester.edu
Urticaria is characterized by the presence of wheals (hives), angioedema or both, and is considered chronic if symptoms are present for 6 weeks or longer (1, 2). Understanding the clinical manifestations associated with chronic urticaria (CU) and its subtypes, and the available treatments will improve diagnosis and better guide clinical management. Therefore, the objective of this article is to highlight the burden of CU, provide evidence-based recommendations to obtain an accurate diagnosis, and outline management strategies.
CU can be broadly divided into urticarias, characterized by the spontaneous onset of signs and symptoms, or inducible/physical urticaria, for which signs and symptoms arise following exposure to specific eliciting factors such as sustained pressure (delayed pressure urticaria) or hot or cold environments (heat- and cold-contact urticaria, respectively) (1, 2). It is possible, and in fact quite common, that two or more forms of CU coexist in the same patient (1, 2).
Differences in terminology exist between the international guidelines and the US practice parameters (1, 2). The international guidelines recognize two subtypes of CU: chronic spontaneous urticaria (CSU) and inducible urticaria (1). The US practice parameters include CU with physical triggers, CU for which a cause may be found, and chronic idiopathic urticaria (CIU; including autoantibody-associated urticarias) (2). The terms CSU and CIU are essentially synonymous in most cases and, as such, the term CSU is primarily used in this review because many cited studies were conducted outside of the US.
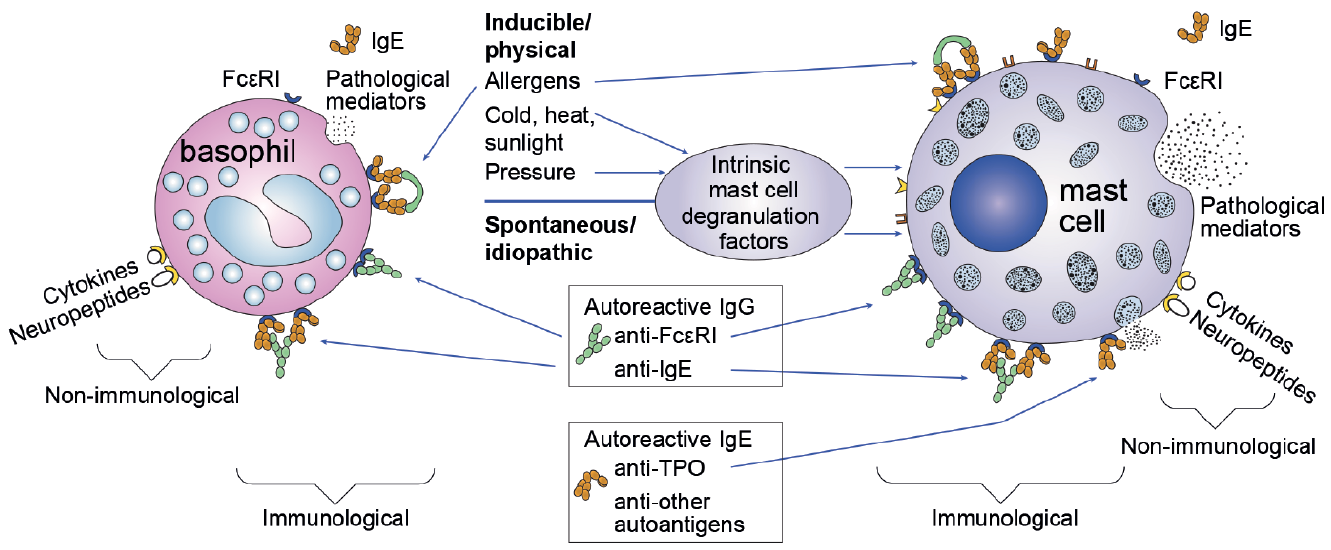
Although the pathology of CU is not fully understood, it is likely that mast cells, basophils, histamine, and other mediators play a key role (Fig. 1) (3–6). The release of histamine and other pro-inflammatory factors following degranulation of mast cells is regarded as the “final common pathway” in both physically induced CU and CSU, and forms the basis of H1-antihistamines as the first-line therapy for CU (4). However, the causative factors leading to degranulation of tissue-resident mast cells or basophils are less clear and likely differ between physically induced CU and autoimmune CU. The autoimmune response is thought to involve autoreactive IgE antibodies against auto-allergens, or autoreactive IgG antibodies against the mast cell (or basophil) high-affinity receptor FcεRI, IgE, or both (4). The concept of a central role for IgE and FcεRI in priming mast cells (or basophils) for degranulation has led to the investigation of novel treatments, such as omalizumab. In the US practice parameters, CIU is considered to have an autoimmune basis in many, but not all, patients, while other underlying causes of CIU that have been proposed, include infections, food intolerance and autoallergy (2, 4). The international guidelines also identify potential causes such as auto-immune disease, hypersensitivity reactions to food and drugs, and infections, but do not differentiate the etiology of CU subtypes (1).
Fig. 1. Pathogenesis of chronic urticaria (CU). CU signs and symptoms develop when skin mast cells or basophils degranulate and release histamine and other proinflammatory mediators. In chronic spontaneous urticaria, the degranulation of these cells in some patients is thought to be due to the effects of autoantibodies directed against a subunit of the high-affinity IgE receptor, FcεRIa, or to IgE itself. Other mechanisms of mast cell or basophil activation that are potentially relevant to CSU involve autoantigens and IgE directed against these autoantigens, as well as complement components, cytokines and neuropeptides. TPO: thyroperoxidase. Adapted from Chang, et al. (4).
Based on a survey conducted in Germany, the lifetime prevalence of CU was estimated to be 1.8% (7). CSU consistently accounts for the majority of cases of CU, with reported estimates ranging from 66% to 93% (8). Many patients remain symptomatic beyond one year, with up to 14% of patients continuing to experience recurrent outbreaks of symptoms for longer than 5 years (9, 10).
The impact of CU on quality of life (QoL) was found to be similar to the impact of ischemic heart disease in patients awaiting coronary artery bypass grafting and greater than respiratory allergy in patients with perennial rhinitis and intermittent asthma (11, 12). Impairment of QoL due to CU was reportedly worse than or similar to that observed with other skin diseases, including psoriasis, acne, or atopic dermatitis (13–15). The impact of CU on QoL has recently been highlighted in an Italian narrative medicine project (16). Based on data from 2004 to 2006, the mean yearly direct and indirect costs of CSU in the US were estimated to be $244 million (17). Of the total annual cost, medication accounted for 62.5% and wages lost because of travel to outpatient visits/absences from work accounted for 15.7% (17).
Impairment of QoL in CSU patients who also have a psychiatric comorbidity (e.g. depression and/or anxiety) has been reported to be greater than in those without a psychiatric diagnosis (18, 19). In a large population-based study, autoimmune diseases (predominantly thyroid disorders) were significantly more common in patients with CU than in control patients without a diagnosis of CU (20).
Well-designed clinical studies have provided evidence for the use of approved doses of second-generation H1-antihistamines as the first-line therapy for CU, and there is broad consensus for such a treatment approach (1, 2). Despite this, a German survey of 776 physicians (43.0% dermatologists, 28.7% pediatricians, and 27.5% general practitioners [GPs]) carried out in 2009 revealed that a considerable proportion reported using sedating antihistamines (23.0%) and oral corticosteroids (17.9%) as the first choice (21). Unfamiliarity with patient management guidelines may have contributed to this observation: physicians who indicated that they were aware of the international guidelines were significantly less likely to use sedating antihistamines than those who were unaware of them (21). Although only one-third of physicians responded that they knew of the international guidelines, there was greater knowledge among dermatologists (50.6%) than among pediatricians (24.2%) and GPs (12.6%) (21). It is noteworthy that in Germany, it is common place for dermatologists to be dual trained in allergy. Therefore, it is possible that knowledge of patient management guidelines among US-based dermatologists may be lower than among German dermatologists.
A cross-sectional survey of 180 healthcare providers in the UK conducted in 2014 reported that 48 of 64 (75.0%) dermatologists used guidelines for the diagnosis and management of CU, compared with 50 of 55 (90.9%) allergists and immunologists. Among these physicians who reported using guidelines, the 2013 international guidelines were cited by a greater proportion of allergists/immunologists (52.1%) than dermatologists (10.6%) (22). Despite this, and in contrast to the earlier German survey, all physicans reported using second-generation antihistamines as first-line treatment.
In an online survey that assessed 80 Canadian dermatologists’ perspectives of CU, most were using H1-antihistamines as a first-line treatment (96.8%). Interestingly, 16.1% of respondents reported > 50% of their patients had refractory CU, and the perceived next best add-on therapy was not consistent. Overall satisfaction with diagnosis and management of CU was low, but most (59.7%) were not familiar with the international guidelines (23).
The knowledge gap is further illustrated by data from a case-series study of referred patients in Denmark who, at presentation to a specialist urticaria clinic in 2009–2011, were generally treated with insufficient doses of second-generation H1-antihistamines (24). The disease management guidelines also show clear consensus on up-dosing second-generation H1-antihistamines in CSU patients who have failed to show sufficient response; however, it was again apparent from the German survey that compared with GPs and pediatricians, dermatologists had the most experience with up-dosing these drugs (21). Nonetheless, even following standard and high doses of second-generation H1-antihistamines a number of patients remain antihistamine-resistant, and it is likely that dermatologists are best positioned to manage these patients. In the German physician survey, dermatologists were found to have more experience of alternative treatment options, such as dapsone and other immunosuppressants, which are of major importance in patients who do not respond to higher doses (21). Understanding what the treatment options are for patients with moderate-to-severe CSU is critical not only for the dermatologists for whom 65.5% of their patients fall into this severity, but also for GPs and pediatricians (with 49.8% and 46.1% patients with moderate-to-severe CSU, respectively) (25).
The international guidelines and US practice parameters both recommend a thorough patient history and physical examination, limited routine laboratory testing, and a stepwise approach to treatment, but they differ in several areas (Tables I, II) (1, 2). For example, the US practice parameters place greater emphasis on the limitations of laboratory testing, discuss treatment options not present in the international guidelines, and do not focus on evaluating treatment success (1, 2).
Table I. Comparison of diagnostic recommendations in the international guidelines and the US practice parameters for the diagnosis and management of chronic urticaria (CU)
Table II. Comparison of recommendations for confirming the relevance and threshold of triggers for inducible chronic urticaria (CU) in the EAACI/GA2LEN/EDF/WAO international guidelines and the US practice parameters for the diagnosis and management of CU
It is worth noting that key similarities and differences between these two important guideline documents have also been considered previously (26). There are few major differences, but where they do occur, it tends to be driven by differences in expert opinion where guidance is provided in the absence of strong scientific evidence (26). Needless to say global consensus activities relating to urticaria are ongoing.
The characteristic skin finding of CU is the presence of hives that typically manifest as edematous, pink or red, pruritic wheals of variable size and shape, and lack any epidermal changes such as scale/crust. Individual lesions are evanescent and typically fade within 24 h. Angioedema generally involves swelling of the lower dermis and subcutis, with frequent involvement of the proximal mucus membranes (ocular or lip edema) or severe peripheral edema. Severe swellings may be painful, and most cases of angioedema typically may take up to 72 h to resolve (1, 2).
As shown in Table I, it is universally recommended to begin the diagnostic process with a thorough patient history and physical examination (1, 2). Where indicated by patient history, provocation tests (e.g. exposure to cold stimulus if cold-contact urticaria is suspected, or use of a dermographometer to elicit symptomatic dermographism) can be used to confirm the relevance and threshold of triggers in patients who have a physical/inducible form of CU (Table II) (1, 2). It is important to note that not all possible causative factors need be investigated in all patients (1). For example, efforts to identify underlying causes should be limited to patients with longstanding and/or severe CSU, although it is important to counsel patients that identifying causes is highly unlikely in the majority of CSU cases (2).
Recommended diagnostic tests and tools may identify CU subtypes and narrow down the differential diagnosis (Table III), but the recommendations are slightly different in each guideline (Table I) (1, 2). Skin biopsies are not necessary for most cases of refractory CU and should be considered only when vasculitis, auto-inflammatory disease or another immunologic condition that can present with hive-like lesions (e.g. bullous pemphigoid, etc.) is suspected (2).
Table III. Conditions to consider in the differential diagnosis of chronic urticaria (CU)
Approved doses of second-generation H1-antihistamines are the universally recommended first-line therapy for CU (1, 2), based on demonstrated efficacy in double-blinded clinical studies (27–31). Because there are not enough comparative studies to identify a preferred agent (1, 2) and individual patients may respond differently to treatment (32), selection must be based on physician/patient discretion. A progressive increase to up to 4-fold the standard dose is recommended for patients who do not respond to approved doses (1, 2). Studies have shown that increasing the antihistamine dose may improve control of CU symptoms, but data for some antihistamines are limited and conflicting (33–41).
In our experience, approximately 50% of all patients with CSU respond to antihistamines at standard doses and another 10–25% will respond with up-dosing, but at CSU referral centers as many as 96% of patients have failed antihistamines even at high doses (42). However, it is important to confirm that the patients have been compliant with the treatment dose and schedule, and that their response is inadequate (43–45). As indicated by both the international guidelines and US practice parameters, additional treatment options are available for patients who do not respond to monotherapy (Fig. 2) (2). Although not included in the international guidelines, the US practice parameters recommend adding an additional second-generation H1-antihistamine and/or H2-antagonist to H1-antihistamine therapy (step 2). Data comparing the efficacy and safety of combination therapy versus up-dosing of a single agent are scarce (46, 47), but, as a general principle, it is likely to be safer to adjust the dosing of a single drug rather than complicating management with several antihistamine classes (48).
Fig. 2. Chronic urticaria treatment algorithm. A) European Academy of Allergy and Clinical Immunology/Global Allergy and Asthma European Network/ European Dermatology Forum/World Allergy Organization (EAACI/GA2LEN/EDF/WAO) international guidelines and B) the US practice parameters for the diagnosis and management of chronic urticaria (CU). NSAID: non-steroidal anti-inflammatory drug. Adapted from Bernstein et al. (2).
First-generation antihistamines have similar efficacy, but greater sedation and impairment compared with second-generation antihistamines, and should therefore be used with caution (1, 2, 28, 29). The US practice parameters recommend the use of first-generation antihistamines at bedtime in order to reduce daytime impairment (2); however, they have been shown to frequently lead to daytime somnolence, sedation, drowsiness, fatigue and impaired concentration and memory, especially if taken late at night (49). H2-antihistamines, specifically cimetidine, used in combination with H1-antihistamines have shown a limited additive effect, and are, therefore, no longer recommended by the international guidelines (50–52).
In the international guidelines and the US practice parameters, patients are considered to have refractory CU based on the absence of clinical response to antihistamine therapy. However, the international guidelines consider the threshold to be up to 4 times the approved dose of antihistamines, whereas the US practice parameters consider it to be maximal combination antihistamine therapy (1, 2). Similarly, the treatment course for patients non-responsive to antihistamine treatments differs between the international guidelines and US practice parameters (1, 2). For these patients, a number of treatment options are available, several of which have evidence from at least one double-blind randomized controlled trial that supports their use (Table IV) (1, 2, 45, 53, 54).
Table IV. Agents with at least one double-blind randomized controlled trial supporting its use for patients with refractory chronic urticaria (CU) who are resistant to high-dose or combination antihistamine therapy
Oral corticosteroids are frequently used in patients with CU not adequately controlled with antihistamine therapy, yet no controlled study has been performed (2, 55). A large retrospective study found that 50% of patients with antihistamine-resistant CU treated with a single course of prednisone (25 mg/day for 3 days, de-escalated to 12.5 mg/day for 3 days and 6.25 mg/day for 4 days) had a remission, and an additional 9% responded after a second course (56). The main concern with the use of corticosteroids is the risk of adverse effects, thus only short-term use to help manage exacerbations should be considered (1, 2).
Leukotriene-modifying agents (LTMAs) such as montelukast and zafirlukast, are reportedly effective for the treatment of CU as monotherapy or in combination with H1-antihistamines, with the strongest evidence for montelukast (10 mg/day), although the treatment effect observed was small (57–65). Results of clinical studies have been inconsistent; some showing superiority (60, 64, 65), and others demonstrating inferior responses from LTMAs compared with antihistamines (61), or even a lack of efficacy compared with placebo (66).
Agents with H1- and/or H2-antagonist activity such as hydroxyzine, cyproheptadine, or doxepin are also options for patients whose symptoms do not respond to prior antihistamine therapy, but they have considerable sedating effects (1, 2). Compared with other antidepressants such as amitriptyline, nortriptyline, and mirtazapine, clinical evidence is strongest for doxepin (at doses from 10 mg to 25 mg 3 times daily) (2, 32, 67–69); however, sedation, electrocardiographic effects at doses >100 mg, and numerous drug–drug interactions may limit its use (2, 70, 71).
Of the available agents recommended for patients with refractory CU, omalizumab (Xolair®, Genentech, Inc.; San Francisco, CA), an anti-IgE antibody, has the most robust data supporting its use (45), and as of February 2016 is the only agent approved by the US Food and Drug Administration and the European Medicines Agency for the treatment of adults and adolescents who have refractory CIU and CSU, respectively (72, 73). Although omalizumab (administered as subcutaneous injections every 4 weeks at doses of 150 mg, or 300 mg) has a favorable risk/benefit ratio and was well tolerated in clinical studies (74–76) it has infrequently been associated with ana-phylaxis (72, 76). Omalizumab has also been shown to be an efficacious treatment alone or as an add-on therapy to H1-antihistamine plus an H2-antihistamine or LTMA, or a combination of these for patients with CIU refractory to antihistamine treatment in 3 Phase 3 studies (74–76). However, the cost of treatment, the requirement for subcutaneous administration in a physician’s office and anaphylaxis concerns may limit its use (2, 45).
In addition to omalizumab, both the international guidelines and the US practice parameters recommend consideration of cyclosporine A (CsA) for patients with refractory CU (1, 2). CsA is an immunosuppressant that has been shown to be an effective treatment for CU (at dosages of 3–5 mg/kg/day for up to 4 weeks) in placebo-controlled studies as a solo treatment and in combination with second-generation H1-antihistamines (77, 78). Treatment with CsA is associated with a relatively high incidence of mild adverse effects including gastrointestinal disturbances, paresthesia and infections (77, 78); retrospective study showed that adverse effects were generally mild and transient for patients with CU using low-dose CsA (< 3 mg/kg/day) for up to 10 years (79). However, long-term, low-dose CsA treatment is known to be associated with nephrotoxicity (80). Clinicians need to carefully consider whether CsA is an appropriate treatment option based in part on a patient’s comorbidities. For example, subjects with hypertension and/or renal insufficiency would not be a good candidate for CsA treatment. It is also important to be aware that there are clinically important differences in bioavailability between CsA preparations (2, 81, 82).
Additional anti-inflammatory agents and immunosuppressants can be considered for patients with refractory CU (2), but there is limited evidence supporting the use of these agents (44, 83, 84). Anti-inflammatory agents, including dapsone, sulfasalazine, hydroxychloroquine and colchicine, have limited evidence for efficacy in CU (2), but a recent double-blind, placebo-controlled study in patients with CSU indicates dapsone 100 mg/day led to a significant improvement of symptoms (85). It remains to be confirmed whether these agents are more effective in patients with neutrophil-rich urticaria. An open study reported that among CU patients with neutrophilic skin inflammation, 8 of 9 treated with colchicine and 3 of 3 treated with dapsone showed a response (2, 86). Other immunosuppressants to consider include tacrolimus, mycophenolate and methotrexate, but clinical evidence supporting their use is very low (2). Case reports suggest that the anti-CD20 biologic, rituximab, may also provide some benefit (87). A recent publication assessing treatment response in relation-ship to CU characteristics may be useful for selecting treatment regimens (57). More studies, especially randomized controlled trials, are needed to confirm the clinical improvement seen with these off-label therapies, as well as comparative effectiveness studies of both FDA-approved and off-label therapies. There is still an unmet need for new, more effective therapies to treat patients with refractory CU and with this greater refinement of which CU sub-phenotypes will respond best to which therapy.
The goal of CU treatment is to achieve substantial improvements in symptoms with limited adverse effects (1). It is important to measure the patient’s urticaria activity at baseline, and during subsequent visits to the clinic in order to objectively assess the response to treatment(s). The Urticaria Activity Score (UAS) is a validated tool (87, 89) that has been used frequently for measuring and monitoring disease activity in clinical studies of urticaria and clinical practice (1, 74–77, 90, 91). In the international guidelines, the sum of the patient-reported UAS over 7 days (UAS7) is the recommended approach for assessing treatment success in CSU (Table I) (1, 88).
The Urticaria Control Test (UCT) is an alternative patient-reported instrument validated for retrospective assessment of any CU subtype using 4 questions (92). Visual analog scales can also be used to assess disease severity and response of symptoms to treatment that are difficult to measure objectively, such as itch intensity (93).
Because of the significant impact CU has on QoL, assessing QoL is an important aspect of monitoring disease activity (1). The Dermatology Life Quality Index (DLQI) is a validated 10-question tool to compare QoL in patients with a variety of skin conditions that has correlated positively and significantly with UAS (15, 88). The Chronic Urticaria Quality of Life Questionnaire (CU-Q2oL) is a validated QoL tool and the only disease-specific QoL instrument recommended for patients with CSU (1, 89, 94, 95). The UAS and CU-Q2oL should be used to measure the effects of change in CSU disease activity rather than non-validated tools (96).
CU is a complex disorder that has a substantial economic burden and a significant impact on patients’ QoL. A complete history and physical examination will ensure the accurate diagnosis of CU and will determine the extent of laboratory studies needed for each individual patient. Many patients may respond adequately to approved doses of second-generation H1-antihistamines, which should be first-line therapy. For those who does not achieve significant clinical improvement, the advice is to increase the dose of these non-sedating antihistamines to up to 4 times the approved dose. The authors recommend using one antihistamine in this category for the dose escalation rather than double the dose of two different second-generation antihistamines. During this dose escalation the addition of a sedating antihistamine in the evening can also be effective, but combining a non-sedating antihistamine and a sedating antihistamine is not recommended by all experts or the EAACI/GA2LEN/EDF/WAO guideline. If dose modulation of the first- and second-generation antihistamines do not significantly improve the CU and/or if the side effects needed to achieve this level of clinical improvement are unacceptable then one should consider the addition of omalizumab. If omalizumab fails, is not well tolerated or unavailable, alternate options should be considered: CsA, dapsone, colchicine, mycophenolate, sulfasalazine, rituximab or leukotriene antagonists. Of these options the evidence of clinical effectiveness is most robust for omalizumab and to a lesser extent CsA. The advantages and disadvantages of each of these options should be taken into consideration when selecting an appropriate therapy.
Conflicts of interest: LAB is a consultant for AbbVie, Array Biopharma, Celgene, Genentech, MedImmune, Novartis, and Regeneron. JAB has received research funding from Novartis and Genentech and is a speaker and consultant for Novartis and Genentech. MM is or recently was a speaker and/or advisor for FAES Farma, Almirall Hermal, Genentech, GlaxoSmithKline, Merckle Recordati, Novartis, Sanofi Aventis, Merck Sharp & Dohme, Moxie, Takeda, UCB, and Uriach.
Disclosure and funding sources: Medical writing and editorial assistance in the development of this manuscript were provided by Sarah Thornburg at JK Associates, Inc., Conshohocken, PA, USA, a part of the Fishawack Group of Companies, and this service was supported by Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA and Genentech, Inc., South San Francisco, CA, USA.


 Click to show fullsize
Click to show fullsize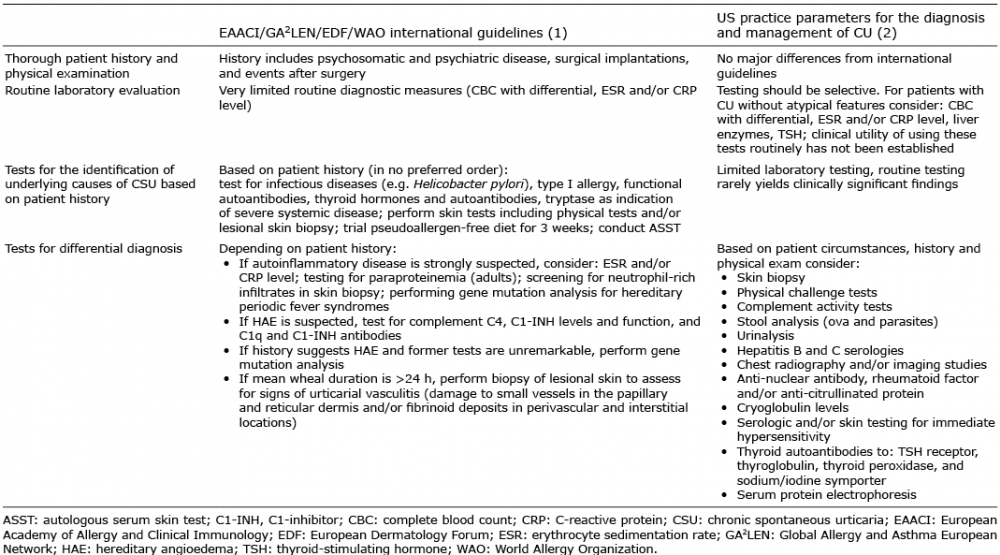 Click to show fullsize
Click to show fullsize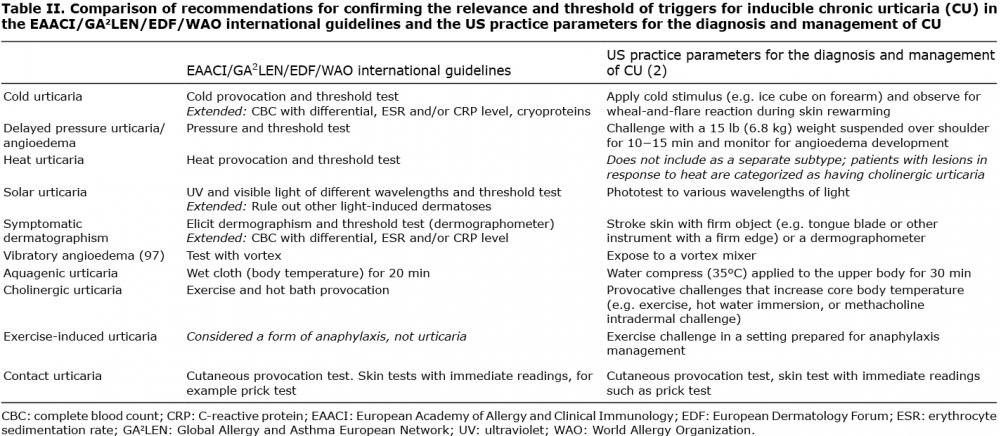 Click to show fullsize
Click to show fullsize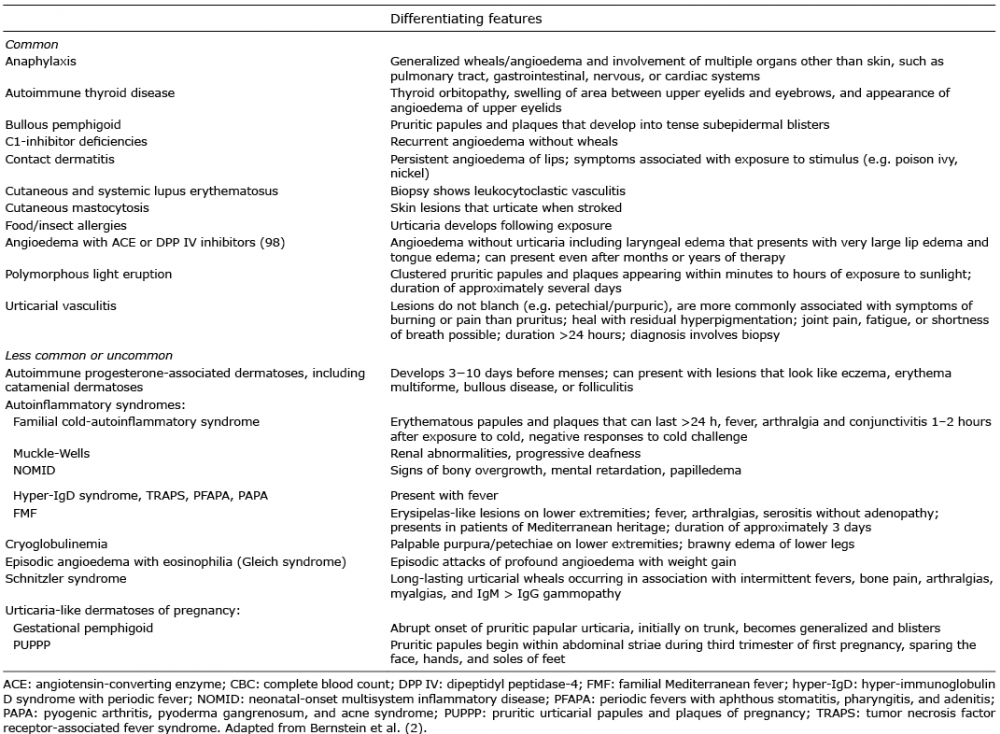 Click to show fullsize
Click to show fullsize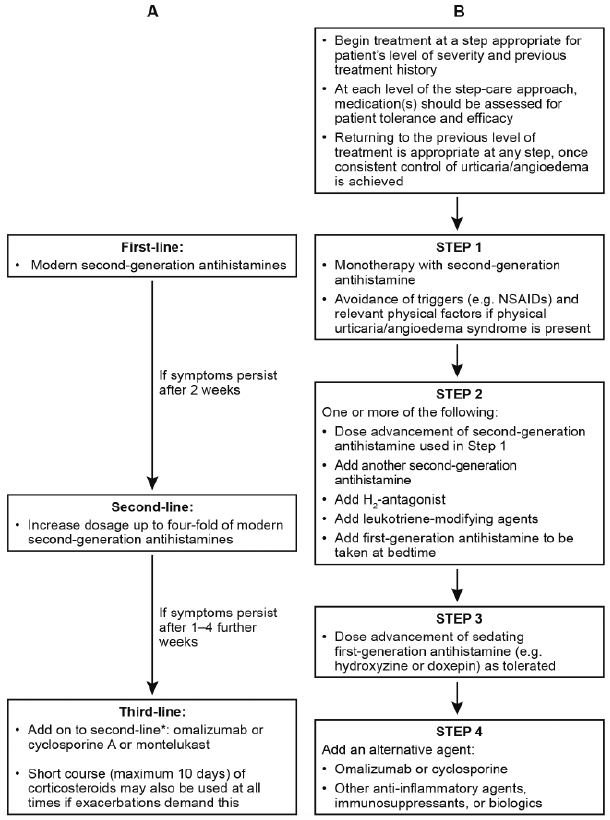 Click to show fullsize
Click to show fullsize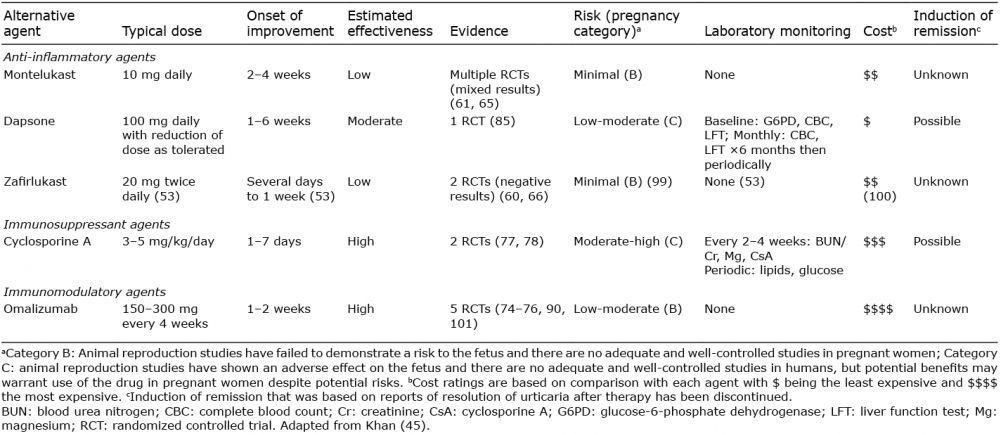 Click to show fullsize
Click to show fullsize