


1Unit of Dermatology, University of Padua, Via C. Battisti 206, IT-35128 Padua, and 2Department of Pathology, San Bortolo Hospital, Vicenza, Italy. E-mail: mauro.alaibac@unipd.it
Accepted Jul 4, 2016; Epub ahead of print Jul 5, 2016
Primary cutaneous lymphomas (PCLs) are classified as a type of non-Hodgkin’s lymphoma (NHL). They are the second most common group of extranodal NHLs after the gastrointestinal lymphomas, with a global annual incidence of approximately 1/100,000 in Western countries (1). PCLs include cutaneous T-cell lymphomas (CTCLs), which constitute approximately 75–80% of all PCLs, and cutaneous B-cell lymphomas (CBCLs), which represent approximately 20–25% of all PCLs (2). Mycosis fungoides (MF) is the most common type of CTCL, whereas primary cutaneous CD30+ lymphoproliferative disorders (CD30+PCLPDs) are the second most common type.
Within the group of CD30+PCLPDs, lymphomatoid papulosis (LyP) and cutaneous anaplastic large cell lymphomas (C-ALCL) can be distinguished (2). Both LyP and C-ALCL have an excellent prognosis (3). LyP is an indolent lymphoproliferative disorder clinically characterized by recurrent papulonodular lesions, which undergo spontaneous regression (4). Histologically, 6 types (A–F) of LyP with different histopathological and clinical features have been described (5–8). C-ALCL generally presents clinically with solitary or localized ulcerating tumours or nodules, although multifocal distribution of lesions are described in 20% of cases (9). Histologically C-ALCL are characterized by a diffuse non-epidermotropic infiltrate with more than 75% of cells positive for CD30 (10). Treatment of LyP usually involves low-dose methotrexate (MTX) and ultraviolet (UV) phototherapy, whereas localized radiotherapy and surgical excision are commonly used for treatment of C-ALCL (3). Recently, a variant of C-ALCL, characterized by an angiocentric/angiodestructive pattern and cytotoxic phenotype, has been described (11).
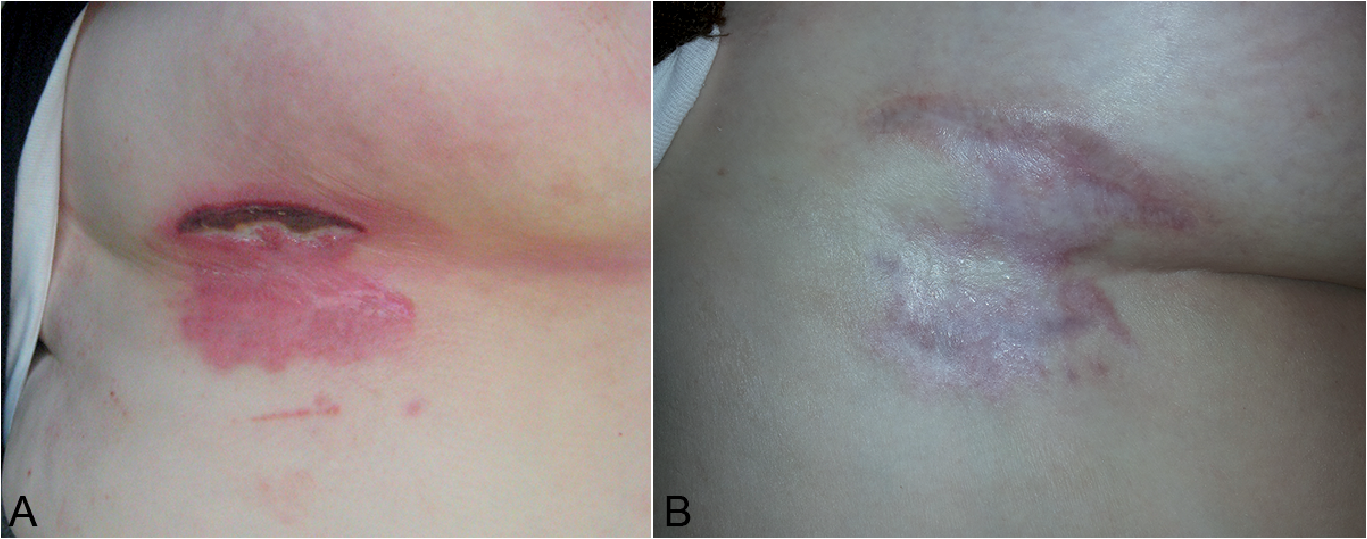
A 72-year-old woman presented with a solitary flat nodule of the right inframammary fold, evolving into an eschar-like necrotic plaque with a mean diameter of 15 cm. A few months before the patient presented to our Dermatology Unit, she had started to develop an itching erythematous patch in the right inframammary area, which soon became red, swollen and ulcerated and was initially diagnosed as submammary intertrigo.
When the patient presented to our Dermatology Unit, she had a deeply painful ulcerated lesion of the right inframammary fold (Fig. 1A). Complete blood cell count, liver and kidney function tests and lactate dehydrogenase were normal. The patient had no comorbidities except for a stenosis of the right internal carotid artery treated with stents; she took acetylsalicylic acid and clopidogrel once a day. We performed a skin biopsy and a microbiological swab test, which was positive for Proteus vulgaris sensitive to penicillin. Histological examination revealed a central necrosis surrounded by an atypical infiltrate of medium-to-large-sized atypical lymphoid cells extending into the subcutis and characterized by an angiocentric pattern. The infiltrate was composed of CD4+ cells, which included approximately 80% of atypical CD30+ lymphoid cells (Fig. 2). Any involvement of systemic lymphoma was excluded by PET/CT. The histopathological features, correlated with the clinical appearance of the lesion, conformed to the newly described angioinvasive C-ALCL. The patient was treated systemically with methotrexate, 10 mg/week, and topically with 1% silver sulphadiazine solution. Regression of the lesion was observed within 6 weeks. After 4 months from the beginning of MTX, blood count, kidney and liver function were normal and complete remission was achieved (Fig. 1B). Thus, we decided to stop MTX. At the present, after 18 months from the diagnosis and 14 months from the complete remission, the patient continues with regular follow-up and there is no evidence of disease.
Fig. 1. (A) A deeply painful ulcerated lesion on the right inframammary fold. (B) Complete remission of the cutaneous lesion after 4 months.
Fig. 2. (a) Low-power view of skin specimen showing central necrosis surrounded by an atypical infiltrate extending into the subcutis and characterized by an angiocentric pattern (× 10). Inset: high-power view of the neoplastic cells.
An eschar-like ulcer developed on a pre-existing nodule may be observed in LyP type E, also known as angioinvasive LyP, or in C-ALCL (11). These 2 different conditions cannot be distinguished histopathologically (11). Neoplastic cells are pleomorphic or anaplastic, medium- to-large-sized, with prominent nucleoli and constitute a diffuse or perivascular infiltrate. An angiocentric/angio-destructive infiltrate is always found in the dermis with destruction of small-to-medium-sized vessels, fibrin deposits and intraluminal thrombi (11). LyP type E is generally characterized clinically by the appearance of new lesions and regression of others, whereas a solitary ulcerated lesion covered by black eschar characterizes C-ALCL with angioinvasive features. In our case, histological examination revealed a diffuse infiltrate of medium-to-large-sized atypical lymphoid cells expressing CD30 with distinct angioinvasion and angiodestruction greatly resembling angioinvasive LyP type E. The presence of a solitary nodule at the initial presentation and the absence of spontaneous regression during the first 6 weeks from its appearance led us to perform the diagnosis of C-ALCL with angioinvasive features. At initial presentation is very important to differentiate these 2 forms; LyP usually presents with multiple papular lesions; whereas C-ALCL presents with a single large lesion, although a few cases of angioinvasive LyP presenting initially with a solitary lesion have been described (11) and multifocal distribution of C-ALCL lesions has been reported (9). Thus, sometimes LyP type E and the new ALCL variant may be distinguished only during the follow-up. The typical course of LyP consists of occurrence of new lesions and regression of others within a few weeks while C-ALCL is usually a single persisting lesion (8). Rare cases of C-ALCL followed by LyP or concomitant occurrence of large solitary lesions resembling C-ALCL and small recurrent papular lesions typical of LyP have been reported in the same patient (12). C-ALCL should also be differentiated from unilesional MF, which may be characterized by a slow transition from the initial patch/plaque stage to the nodular stage. Surgical excision and radiotherapy are the best documented therapies for localized angioinvasive C-ALCL (11). Because of the size and location of the lesion in our case, surgical excision was not possible. Furthermore, radiotherapy was not indicated because of the presence of deep ulceration. Thus, we preferred to use systemic low-dose MTX, although there are only anecdotal reports on its use in C-ALCL, whereas it is widely used for LyP (13, 14). Our treatment approach could be considered innovative and effective, leading to a complete clinical response within a few months.
In conclusion, the diagnosis of LyP type E and angio-invasive C-ALCL sometimes overlaps, demonstrating that these 2 different conditions effectively represent a clinicopathological continuum.


 Click to show fullsize
Click to show fullsize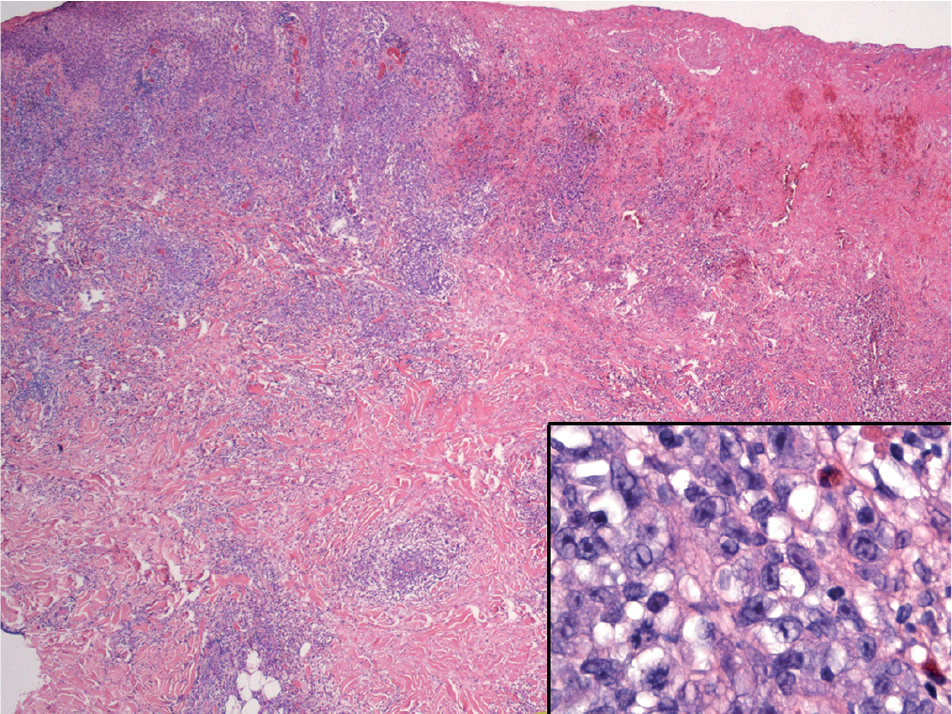 Click to show fullsize
Click to show fullsize