


1Service de Medecine Interne, Hôpital Bretonneau, 2 Boulevard Tonnelle?, FR-37044 Tours, 2Service de Chirurgie Vasculaire, Hôpital Trousseau, CHRU of Tours, 3Service de Dermatologie, Hôpital Trousseau, Tours, 4Service de Dermatologie, Gustave Roussy campus cancer, Villejuif, and 5Université François Rabelais, UMR GICC 7292, Tours, France. *E-mail: bertrand.lioger@univ-tours.fr
Accepted Jul 4, 2016; Epub ahead of print Jul 5, 2016
Therapeutic management of metastatic melanoma is undergoing a revolution, with the use of immune-checkpoint inhibitors, such as anti-cytotoxic T-lymphocyte antigen 4 (CTLA-4) and anti-programmed cell death 1 (PD-1) antibodies. Along with a significant durable efficacy of these therapies (1–3) a new class of adverse events has emerged, namely immune-related adverse events (irAEs). Hypophysitis, thyroiditis, rashes, autoimmune colitis, and autoimmune hepatitis represent such side-effects. In safety studies, these severe irAEs have accounted for less than 15% of overall side-effects (4–6). We report here a case of arterial thrombosis and diabetes mellitus in a patient treated with anti PD-1 antibody pembrolizumab (MK-3475).
A 73-year-old man, who had a history of hypertension and right tibial venous thrombosis following a long journey 30 years ago, was admitted for an acute ischaemia of the left lower limb and a diabetic ketoacidosis while he was treated with pembrolizumab, 10 mg/kg/day, every 3 weeks for 26 weeks, for a stage IV melanoma of the scalp with lymph node, cutaneous, bone and liver metastases. He presented with a painful cyanotic and cold left foot (Fig. 1). Pedal and posterior tibial left pulses were abolished. Laboratory tests showed blood neutrophils 19×109/l (normal 2.0–7.0×109/l), platelets count 211×109/l (normal 150-450×109/l), C-reactive protein 37.1 mg/l (normal < 5 mg/l). Fibrinogen clotting tests were normal. Anticardiolipin antibodies, anti-beta2-glycoprotein 1 antibodies, and lupus anticoagulant test were negative and anti-thrombin III was normal. In terms of diabetes mellitus, metabolic acidosis (pH: 7.15 and lactic acid: 2.1 mmol/l) and haemoglobin A1C of 8.5% were found. Both anti-glutamic acid decarboxylase (GAD) and anti protein-tyrosine phosphatase-2 (IA-2) antibodies were negative. Before this episode of diabetic ketoacidosis, the patient showed no sign of diabetes and glucose levels were normal. Computed tomography did not show pancreatitis or pancreas metastasis, but revealed an arterial thrombus floating in the infra-renal aorta (12×5 mm) without atheroma plaque next or distally in the vicinity, associated with an arterial thrombosis from the left tibiofibular trunk to the left anterior tibial artery (Fig. 2). Other vascular axes were free of parietal atheroma, calcified plaque or aneurysm. Heart rate was sinus, and echocardiography was normal. Fogarty arterial embolectomy associated with anticoagulation allowed vascularization to recover. Pathological examination found a fibrin clot with no neoplastic cells.
Fig. 1. Ischaemia of the left foot.
Fig. 2. Computed tomography revealed aortic thrombus floating and arterial thrombosis of the left tibiofibular trunk to the left anterior tibial artery (arrow).
Arterial Echo-Doppler at 3 months showed a complete disappearance of the thrombus. However, despite iloprost infusions and anticoagulation, a distal necrotic evolution of the foot led to a trans-phalangeal amputation. Pembrolizumab was stopped at the onset and has not been resumed to date. Follow-up, including clinical examination, fluorine-18 fluoro-2-deoxyglucose ([(18)F]FDG) positron emission tomography/computed tomography scan every 3 months, revealed a partial melanoma remission with no thrombotic recurrence at 24 months. Diabetes mellitus still required daily insulin. Anticoagulation has been withdrawn at 6 months and arterial thromboembolism prevention with aspirin was started.
This report is the first description of an arterial thrombosis occurring concomitantly with fulminant type 1 diabetes in a patient treated with pembrolizumab for a stage IV melanoma. The risk of thromboembolic disease is increased in patients with cancer, in relation with hypercoagulable state, malnutrition, bed rest, vascular compression, and side-effects of drugs. In a French retrospective study, such risk has been estimated at 25.2% in stage IV melanoma (7). However, only venous thrombotic events have been described in the literature (8). In our patient, usual causes of arterial thrombosis, including embolic heart disease, atherosclerosis, aortic or popliteal aneurysm, acquired thrombophilia, or intra-arterial metastasis have been ruled out. Indeed, in our patient we strongly suggest that arterial thrombosis was linked to the use of anti-PD1, but through a direct pro-thombotic effect. Pro-inflammatory and pro-atherogenic effects of anti-PD1 were reported in a mouse model (9). However, no atheroma plaque was demonstrated as causal occurrence of thrombosis in the patient. Moreover, direct prothrombotic effect has not been demonstrated and no thrombotic event related to anti-PD1 agents has been reported during phase I/II or III trial (5, 6). A second “hit” or trigger may be necessary to promote thrombosis.
The spectrum of endocrinopathies induced by immune-checkpoint inhibitors has been growing up with the recent description of fulminant type 1 diabetes associated with anti-PD1 antibodies (10). Previous reported cases exhibited atypical features compared with classical type 1 diabetes, such as a late age onset (>55 years), the absence of immunological markers of diabetes in half of the patients, sometimes associated with a high-risk human leucocytes antigen type for developing type 1 diabetes, and simultaneous autoimmune thyroiditis in 2 patients (10–12). As the appearance of thrombosis was concomitant with diabetes mellitus in our patient, we figured out that both adverse events should be related. Indeed, a procoagulant tendency was shown in diabetic patients, especially in ketoacidosis, due to endothelial dysfunction, oxidative stress increase and pro-coagulant changes in clotting factors (13–15). We estimate that ketoacidosis, which occurred concomitantly with arterial thrombosis, and which has been demonstrated to increase the risk of both arterial and venous thrombosis, was the triggering factor of arterial thrombosis in our case.
Thus, we recommend thromboembolism prevention in cases of pre-existing diabetes, and particularly as regards ketoacidosis, in patients under pembrolizumab therapy. As our case was the first description of an arterial thrombosis, we consider this event to be an indirect irAE. However, other similar cases are needed to confirm our hypothesis.
Conflicts of interest: CM and CR were involved as investigators in clinical trials involving melanoma and pembrolizumab. CR advisory board: BMS, GSK, Merck, Roche. The other authors declare no conflict of interest.


 Click to show fullsize
Click to show fullsize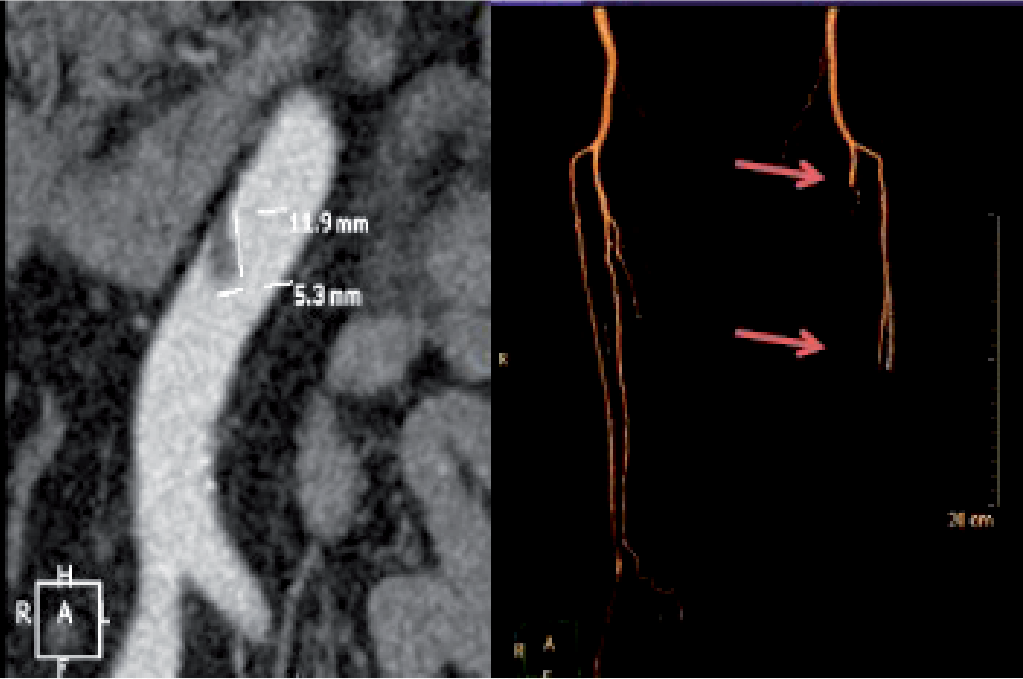 Click to show fullsize
Click to show fullsize