


Departments of 1Dermatology and 2Pediatrics, Gifu University Graduate School of Medicine, 1–1 Yanagido Gifu, 501–1194, 3Department of Technology Development, Kazusa DNA Research Institute, Kisarazu, and 4Department of Dermatology, Fujita Health University, Aichi, Japan. *E-mail: marikoseishima@yahoo.co.jp
Accepted Jul 4, 2016; Epub ahead of print Jul 7, 2016
Pyoderma gangrenosum, acne and suppurative hidradenitis (PASH) syndrome (1) is described as an autoinflammatory disorder, similar to pyogenic sterile arthritis, pyoderma gangrenosum and acne (PAPA) syndrome, but without joint involvement, thereby satisfying the criteria of a disease entity distinct from infection, allergy and autoimmune disorders (2). A specific genetic mutation underlying PASH syndrome has not yet been identified.
Treatment strategies for PASH syndrome and their efficacy have not been well documented. We report here a case of PASH syndrome that was successfully treated with granulocyte and monocyte adsorption apheresis (GMA) therapy, followed by adalimumab.
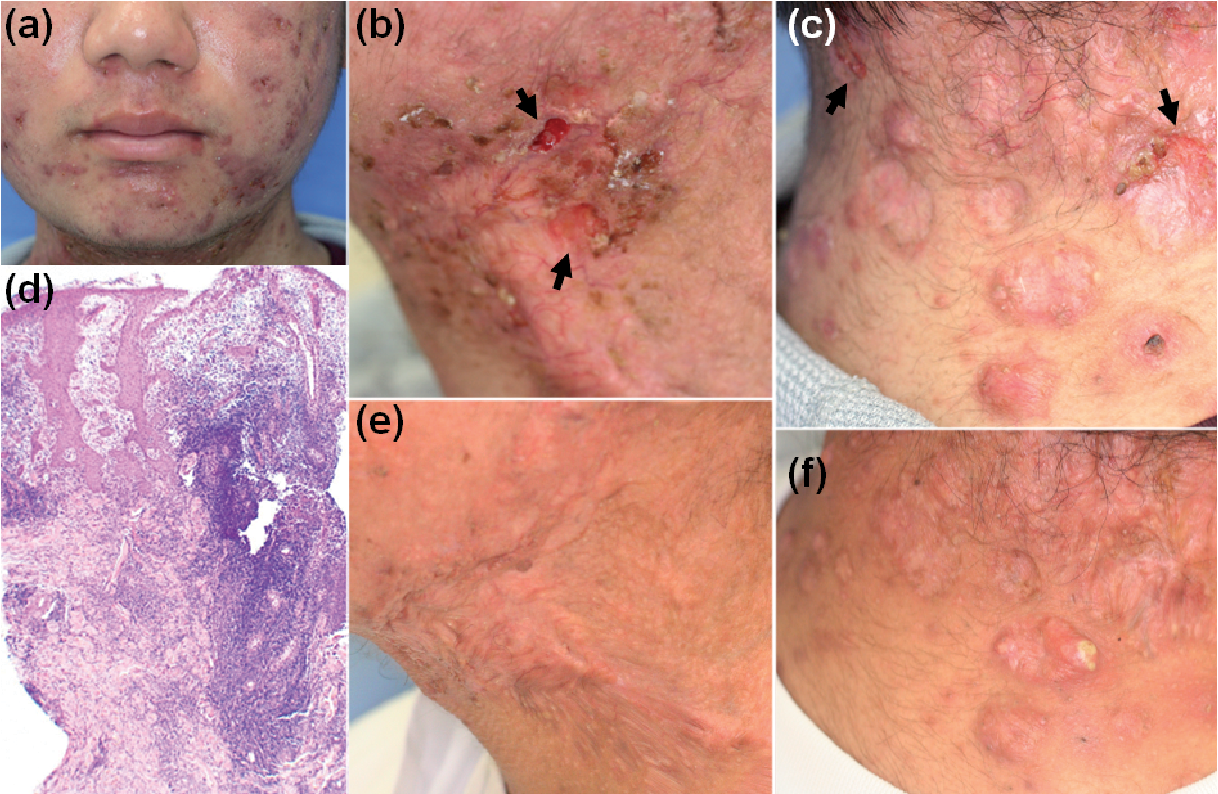
An 18-year-old man was referred to our department with a 2-year history of fever, severe facial pustules and papules, repeated ulcer formation, and scars, accompanied by pain on the neck and occipital region. His medical history included bilateral coxitis for one month at 3 years of age. Suppurative hidradenitis had recurred on his left axilla since 10 years of age. Histological findings of a biopsy specimen obtained from the left neck included infiltration of neutrophils in the whole dermis, especially around the follicle (Fig. 1d). Considering these findings, a diagnosis of pyoderma gangrenosum was suspected, based on which the patient was treated with prednisolone (PSL), 30 mg/day for 4 weeks. However, PSL, cyclosporine, dapsone, and minocycline were not effective. At the first consultation with our department, we observed severe painful facial pustules and papules (Fig. 1a), as well as ulcers and scars on the left neck (Fig. 1b) and occipital region (Fig. 1c), associated with low-grade fever despite oral administration of PSL, 20 mg/day for 5 months; the patient also complained of pain in the neck and occipital region. Furthermore, many scars were observed on the chest, back and thighs. Laboratory data showed an increased leukocyte count (24,110 /μl) and an elevated C-reactive protein (CRP) level (10.19 mg/dl). No significant pathogenic mutations were detected in the 12 genes associated with known autoinflammatory diseases, PSTPIP1, IL1RN, MEFV, MVK, NLRP12, NLRP3, NOD2, PSMB8, TNFRSF1A, NLRC4, PLCG2 and HMOX1. Bacteria were not detected in the ulcers or pustules. The patient has no siblings, and his parents do not have any similar symptoms. The results of osteoarticular and intestinal examinations were normal. Considering the findings, a diagnosis of PASH syndrome was made on the basis of the clinical features of pyoderma gangrenosum, pustular acne and suppurative hidradenitis. The patient received GMA sessions weekly for 10 consecutive weeks. The flow rate was 30 ml/min, and the duration of each GMA session was 60 min.
Fig. 1. Clinical findings on (a) the face, (b, e) left neck and (c, f) occipital region. (a–c) At the first consultation. (e, f) After granulocyte and monocyte adsorption apheresis therapy. Arrows show ulcer formation. Histological findings of the neck show infiltration of neutrophils in the whole dermis, especially around the follicle (haematoxylin and eosin staining; original magnification, ×200).
After 2 sessions, the ulcers on the neck (Fig. 1e) and occipital region (Fig. 1f) and the low-grade fever and pain disappeared, and the number of pustules, swelling and erythema on the face and neck were remarkably reduced. The CRP level significantly decreased to 1.89 mg/dl after the 3rd GMA session and 0.25 mg/dl after the last session. The dose of PSL was reduced to 17.5, 15 and 12.5 mg/day after the 3rd, 8th and last GMA session, respectively. However, pustule formation did not completely disappear. Therefore, adalimumab administration was initiated 1.5 months after GMA, 40 mg/day bi-weekly. Symptoms improved 2 weeks after the first adalimumab injection, but pustule formation continued despite 14 injections, including a dosage increase to 80 mg bi-weekly.
Pyoderma gangrenosum is a neutrophilic inflammatory disease with an unidentified pathogenesis. It is frequently associated with inflammatory bowel diseases (IBD) and/or suppurative hidradenitis. Autoinflammatory syndromes, such as PASH (1, 2), PAPA (3), pyogenic sterile arthritis, pyoderma gangrenosum, acne and suppurative hidradenitis (PAPASH) (4), and pyoderma gangrenosum, acne, suppurative hidradenitis and seronegative spondyloarthritis (PASS) (5) syndrome may be categorized on the same spectrum. Although PAPA syndrome is thought to be caused by an elevation of interleukin (IL)-1β due to mutations in the PSTPIP1 gene, underlying genetic mutations have not yet been identified in the other diseases. The genetic mutations may involve disruption of key regulators of the NLRP3 inflammasome or other signalling pathways that regulate the activation of inflammatory caspases (2, 6). In our patient, a diagnosis of PASH syndrome was made based on clinical features, namely pyoderma gangrenosum, pustular acne and suppurative hidradenitis without arthritis. However, if arthritis is observed in the future, the diagnosis may be changed to other autoinflammatory disease.
GMA is a type of extracorporeal therapy, using a column filled with cellulose acetate beads that adsorbs activated granulocytes and monocytes, which are effector cells that modulate inflammation in inflammatory diseases (7). GMA is effective for IBD (7), pustular psoriasis (8), pyoderma gangrenosum (9) and other skin diseases (10). However, to our knowledge, this is the first report to show that GMA is effective for treating PASH syndrome.
Treatments such as anti-tumour necrosis alpha antibodies, anti-IL-1 receptor antibodies, cyclosporine and systemic steroids have been administered to patients with PASH syndrome. Although one patient showed complete remission with the combination of infliximab, cyclosporine and dapsone (2), most treatments were minimally effective, with only some patients showing partial remission (6). In the current case we clearly demonstrate that GMA was effective for treating a case of PASH syndrome, although complete remission was not obtained and treatment was continued with adalimumab.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize