


1Department of Dermatology, Medical Research Center, PEDEGO Research Group, University of Oulu and Oulu University Hospital, 2Institute of Health Sciences, Faculty of Medicine, University of Oulu, Unit of General Practice, Oulu University Hospital, and 3Institute of Health Sciences, Faculty of Medicine University of Oulu, Oulu, Finland
Having multiple melanocytic naevi (> 50 naevi) is one of the strongest risk factors for melanoma. However, the epidemiology in adults is unclear. This comprehensive dermatological status investigation of 1,932 birth-cohort study cases aged 46 years analysed the prevalence of multiple melanocytic naevi and their association with sex, socioeconomic status (education) in childhood and adulthood, skin type and sunbathing habits. The prevalence of multiple melanocytic naevi was 11.6% (223/1,930). Higher education (odds ratio (OR) 2.11, 95% confidence interval (95% CI) 1.51–2.96), male sex (OR 1.48, 95% CI 1.07–2.06), sun-sensitive skin type (OR 2.09, 95% CI 1.34–3.27) and regular use of sunscreen (OR 2.03, 95% CI 1.23–3.37) were associated with increased risk of multiple naevi. Inflammatory skin diseases decreased (OR 0.49, 95 CI% 0.33–0.72) the risk of multiple naevi. In conclusion, several risk factors were found for multiple naevi among adults living in high latitudes, in Northern Finland.
Key words: melanocytic naevi; sun exposure; education; risk factors; adulthood; epidemiology.
Accepted Jul 4, 2016; Epub ahead of print Jul 7, 2016
Acta Derm Venereol 2017; 97: XX–XX.
Corr: Suvi-Päivikki Sinikumpu, Department of Dermatology, Oulu University Hospital, P. B. 20, FIN-90029 Oulu, Finland. E-mail: suvi-paivikki.sinikumpu@oulu.fi
Melanocytic naevi are the most common skin finding in adults (1–3). Histologically, they are a local collection of benign melanocytes (4), classified as congenital or acquired (4, 5). The number of melanocytic naevi increases with age in childhood and early adulthood and then start to decrease after middle age (6). Almost all adults present with at least 1 naevus (3). A higher risk of naevi is associated with both male sex and fair skin type (5). Both genetic and environmental factors contribute to the development of pigmented naevi (5, 7). Sun exposure, particularly in childhood, is the main known environmental risk factor (8). Correspondingly, people living at lower latitudes show higher rates of naevi than those living far from the equator (9). Increased sun exposure, regular outdoor activities, insufficient protective clothing and frequent holidays in the sun all increase the risk of melanocytic naevi (5, 6, 9). There is some evidence for a connection between a lower number of naevi and inflammatory skin diseases, such as atopic eczema (10, 11). Currently, there is no consensus regarding the association between socioeconomic status and multiple naevi in adults (12).
Despite their benign nature, multiple melanocytic naevi (> 50) increase the risk of melanoma (5, 9, 13, 14) and the risk increases with every additional melanocytic naevus (15, 16). In total, the incidence of cutaneous melanoma has increased worldwide in recent decades (17, 18). Therefore, given that multiple naevi is a known risk factor for melanoma, the aim of this study was to determine the overall prevalence of melanocytic naevi and multiple melanocytic naevi among a middle-aged population. We also analysed the association of education, sex, sun exposure, sunbathing habits and sunburn, skin type, the presence of inflammatory skin disorders, parents’ education and area of residence in childhood (urban vs. rural) with multiple melanocytic naevi in adulthood.
A population-based birth-cohort study of skin diseases was performed, with 1,932 cohort members followed for 45–47 years from birth. A total of 3,181 persons currently living in a given geographical area (in the city of Oulu and within 100 km of it, including rural areas) were invited to attend a clinical skin examination. Participation rate was 60.7% (3). The study population is part of the Northern Finland Birth Cohort 1966 study (NFBC 1966), a longitudinal research programme in the 2 northernmost provinces in Finland that initially included 12,058 live birth children. The whole NFBC 1966 cohort has been evaluated regularly since birth by means of health questionnaires and clinical examinations.
To determine the prevalence of melanocytic naevi, full dermatological status was examined at an out-patient visit. The examination began with visual observation of the whole skin by a specialist in dermatology or an experienced resident. Visually detected skin tumours were further investigated with a dermatoscope, and the number of tumours (< 10, 10–50 or > 50) determined. An inflammatory skin disease was defined as present if atopic eczema, other eczemas or psoriasis was found in the full dermatological status (3). Body mass index (BMI) was determined in order to assess obesity (> 30 kg/m2).
Education is thought to be the most specific indicator of socio-economic status (SES) (19). Information about the education level of the study cases was obtained from the National Education Register (20), supplemented with self-reported questionnaires concerning personal educational history. The majority (61.3%) of the study population had basic or secondary level education, while 38.7% had achieved tertiary level.
SES of childhood families was recognized from the previous research questionnaires and classified into 4 groups (I–IV) for analysis. Childhood area of residence, i.e. town or village vs. countryside, was determined according to maternity care records from the 1960s (21).
Longitudinal risk of sun exposure was acquired from self-reported questionnaires using the following questions: How often have you burned your skin? (> 10 times/≤ 10 times). How often have you travelled abroad for holidays in the sun during the past 10 years? (At least every other year/never or less than every other year). The use of sunblock was evaluated by asking “How often do you use sunblock in everyday living circumstances/abroad? (Regularly/sometimes/never/do not spend time in the sun)”.
Skin type (I–IV) was determined for all cohort members, based on self-reporting using the Fitzpatrick’ criteria: type I comprised the cases who reported that “skin burns always”, type II referred to “skin burns often”, type III was “skin burns occasionally” and type IV was “skin never burns” (22).
The number of naevi was the main outcome; > 50 was classified as multiple naevi. The cross-sectional point prevalence of multiple melanocytic naevi in the cohort at the age of 46 years was determined. The skin types were classified into 2 groups (I–III and IV) for statistical analysis (23).
The χ2 test or Fisher’s exact test were used for categorical variables, and one-way analysis of variance (ANOVA) for BMI. The risk factors associated with naevi were analysed with multivariate multinomial logistic regression analysis. A stepwise backward multivariate multinomial logistic regression analysis was used to identify the most important risk factors for a high number of naevi, and the lowest group of naevi (<10 naevi) was set as a reference. The following risk factors for naevi were analysed: present SES (education) and previous SES (parents’ education), area of residence in childhood, sun-bathing habits (number of sun burns and holidays in sunny locations and the use of sunscreen), obesity and inflammatory skin diseases. Adjusted odd ratios (OR) and 95% confidence intervals (95% CI) were reported as measures of association. All analyses were performed with the statistical package SAS v. 9.4 (SAS Institute, Cary, Northern Canada, USA) and p-value 0.05 was recognized to be statistically significant.
The study was approved by the ethics committee of the Northern Ostrobothnia Hospital District (§94/2011), and performed according to the principles of the Declaration of Helsinki 1983. Written consent for scientific purposes was received in advance from all participants. No identifying details of the study cases were recorded, ensuring complete anonymity.
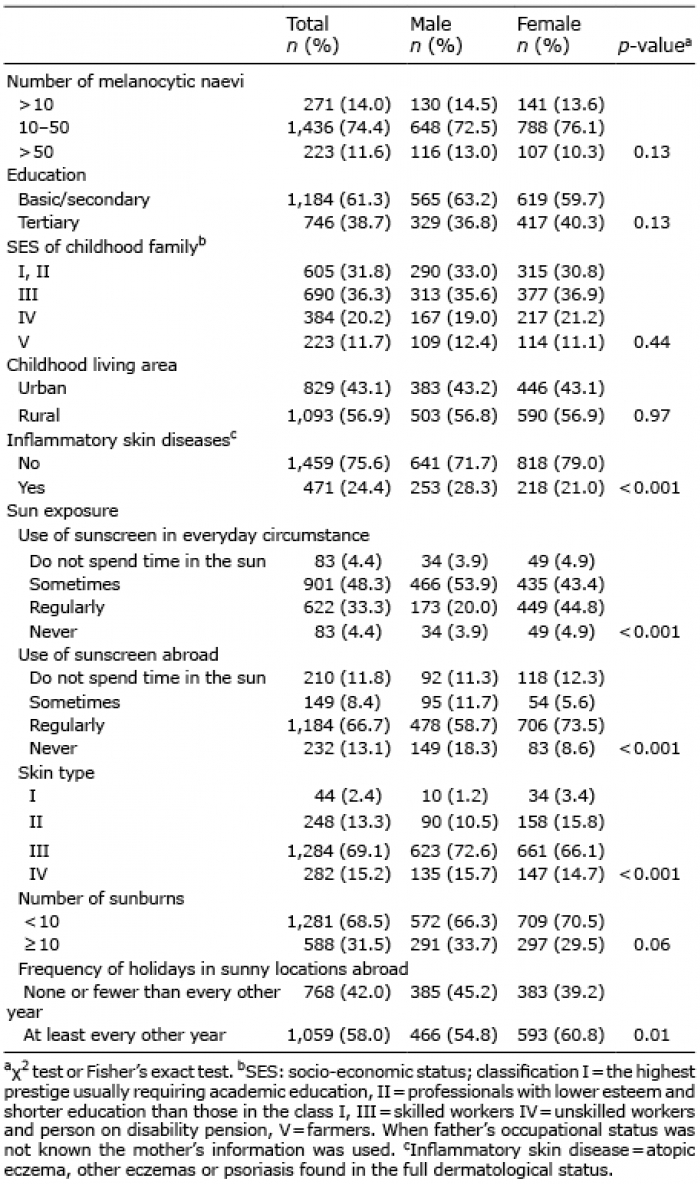
Multiple naevi (> 50 naevi) were present in 11.6% of the study population, 74.4% had 10–50 naevi, and 14.0% had fewer than 10 naevi. Multiple naevi were found in 13.0% of males and 10.3% of females. The majority of the study population had skin type I–III (84.8%), while 15.2% had type IV. The characteristics of the study cases regarding sun-burns and sun-bathing habits are shown in Table I.
Table I. Characteristics of the study population (n = 1,930), the prevalence of multiple melanocytic naevi and sunbathing habits according to sex
Compared with those with higher education (15.5%), the study cases with lower education had significantly fewer multiple naevi (9.0%) (p < 0.001). Those with a higher SES in childhood showed multiple naevi more frequently (13.4%) compared with those with low childhood SES (7.3%, p = 0.02). There was no association between the area of residence during childhood and multiple naevi (Table II).
Table II. Number of melanocytic naevi in the middle-aged study population according to preceding or predictive factors
The prevalence of multiple naevi was 13.9% among those who had had frequent (> 10 times) sun-burn and 10.5% among those who had burned their skin less frequently (≤ 10 times) (p = 0.04). Taking holidays in sunny locations at least every other year was associated with a higher rate of multiple naevi (p = 0.03) compared with those who had travelled abroad less often than every other year during the past 10 years. Multiple naevi were associated with fairer skin type, being present in 12.2% of the cases with skin type I–III, and in 8.9% of the cases with type IV (p = 0.008) (Table II).
Multiple naevi were found in 8.7% of the cases in whom inflammatory skin disease was detected on total body examination, and in 12.5% of those who did not have psoriasis or any type of eczema (p = 0.001). Obesity (BMI > 30 kg/m2) was not statistically significantly associated with multiple naevi.
According to multivariate multinomial logistic regression analyses, higher education (OR 2.1, 95% CI 1.51–2.96), skin types I–III (OR 2.09, 95 CI% 1.34–3.27), regular use of sunscreen (OR 2.03, 95 CI% 1.23–3.37), and male sex (OR 1.48, 95% CI 1.07–2.06) were found to increase the risk of having multiple naevi (Table III, the crude ORs in Table SI). The same risk factors, expect for male sex, were also associated with increased risk of having 10–50 naevi, albeit the corresponding ORs were lower (Table III).
Table III. Statistically significant risk factors of high number of naevi (> 50) in middle-aged adults
In our study population a moderately high proportion (11.6 %) of middle-aged cases living in high latitudes, in Northern Finland, had multiple naevi. In other countries, the frequency of multiple naevi has previously been reported to vary between 1.4% and 31%, being lowest in Asian countries and higher in Australia (7, 24–34). In Europe the prevalence of multiple naevi has been reported in several studies, but the cut-off in these studies is different regarding multiple naevi. For example, in the UK the prevalence was 23%, while over 100 naevi was defined as multiple naevi. The prevalence was 18% in Germany and, in that study, the definition of multiple naevi was set as over 50 (7, 35). The prevalence rate may also diverge greatly within a country; in Northern Sweden the prevalence was 6%, compared with 22% in the southern part of the country (the definition for multiple naevi in both studies was more than 100) (32, 33). As a result of different cut-off in the epidemiological studies of naevi prevalence, the comparison of the studies is difficult. As a conclusion, the number of multiple naevi in Northern Finland is lower than in Central Europe (Germany). In Northern Sweden the reported prevalence was lower than in our study, but it may have been higher, matching our result, if the definition of multiple naevi had been the same. Moreover, study populations vary greatly in terms of age, skin type, inclusion criteria (hospital patients or unselected cases) or study methods (self-reported questionnaires vs. clinical evaluation by nurses or physicians), which also makes the comparison of the reported prevalences difficult.
Melanocytic naevi are a phenotypic trait influenced by both genetic and environmental factors. Twin studies, as well as clinical and epidemiological studies of melanoma families, provide strong evidence for a genetic burden (7, 36–38). Skin type, which is a genetic characteristic, is known to be associated with a higher number of naevi (5, 39–41). Our study supports this by demonstrating a two-fold risk of multiple naevi among the cases with skin type I–III compared with type IV. Regarding sex difference, multiple naevi were substantially more common in males than in females, which is in line with the previous reports (5, 13). This difference may partly be explained by more frequent sunburns and behavioural factors, such as time spent outdoors and clothing in males.
Sun exposure is the main known environmental risk factor for melanoma (8, 13, 16, 34, 39). In our study, up to one in every 3 study subjects had had several sunburns, and more than half of study subjects reported taking frequent holidays in sunny locations. These sunbathing risk factors were associated with a higher count of multiple naevi, which is concordant with previous studies (8, 35, 42). Importantly, intermittent ultraviolet (UV) exposure is more harmful for those who live far from the equator, and are thus not accustomed to intensive sun exposure (5, 9, 33). In previous studies, the relationship between the number of naevi and the use of sunscreen has been controversial. The protective role of sunblock has been reported in children (8, 41), but in adults the use of sunscreen was associated with higher counts of naevi (43), which is also supported by our data, since in our study regular use of sunscreen increased the risk of multiple naevi among adults. This may arise from increased duration of UV exposure due to a false sense of security given by sunblock.
To the best of our knowledge, our data is the first to report a higher prevalence of multiple naevi among highly educated cases compared with the cases with low education level (15.5 % vs. 9.0%). The risk of multiple naevi was increased two-fold among educated cases, even after adjusting for holidays in sunny locations and other sunbathing habits for analyses. This finding has not been reported previously in an adult population (12) or in adolescents (44). Instead, SES is known to associate with melanoma (45, 46), atypical naevi (47) and lifetime UV exposure (48). In our study, a higher rate of multiple naevi was associated with childhood SES (Table SI1), but especially with present SES based on concurrent education. Thus, there should be a focus on preventive interventions against multiple naevi, not only to improve situation among highly educated but also among the next generation.
There are some limitations in the current study. Sunburn, the use of sunscreen, and the number of holidays in sunny locations were self-reported, which may lead to recall bias and incorrect estimation. However, this birth-cohort study with an exceptionally long follow-up has some strengths compared with the existing literature. The participation rate was sufficiently high to result in a large study population. Instead of self-reporting, all study cases were dermatologically investigated by an expert. For each participant, preceding factors were available from the comprehensive study registries since pregnancy.
In conclusion, we found a relatively high proportion of multiple melanocytic naevi among middle-aged birth cohort study subjects. The result is well generalizable in the Caucasian population, especially among those living at high latitudes. High education level, male sex, and light skin type increased the risk of multiple naevi, and therefore, the risk of melanoma. Preventive information about the risks of UV exposure and more healthy sunbathing habits should be highlighted, especially in these risk groups.
This study was supported by Oulu University Hospital, the Northern Finland Cancer Association, the Academy of Finland, the Medical Research Center, University of Oulu, the Finnish Medical Foundation and the Finnish Medical Dermatological Society.
The authors declare no conflict of interest.


 Click to show fullsize
Click to show fullsize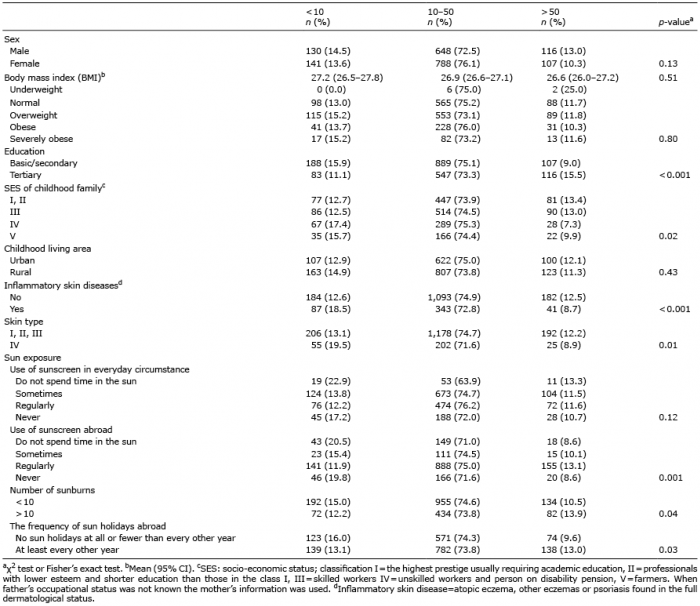 Click to show fullsize
Click to show fullsize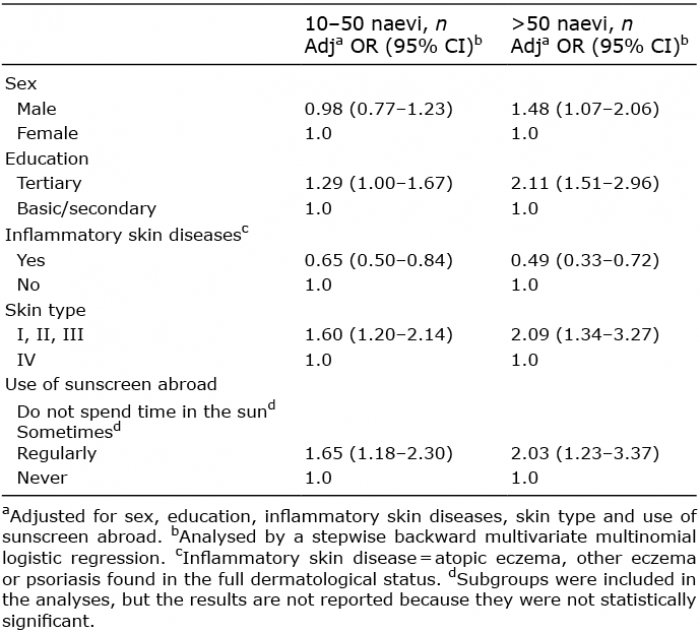 Click to show fullsize
Click to show fullsize