


Departments of Dermatology, 1University of Groningen, University Medical Center Groningen, Hanzeplein 1, NL-9700 RB Groningen, 2Radboud University Medical Center, Nijmegen, 3Deventer Hospital, Deventer, 4Academic Medical Center, Amsterdam, 5Erasmus University Medical Center, Rotterdam, The Netherlands, and 6Member of the European Hidradenitis Suppurativa Foundation. E-mail: b.horvath@umcg.nl
Accepted Aug 16, 2016; Epub ahead of print Aug 18, 2016
Sir,
Hidradenitis suppurativa (HS) is a chronic, recurring, debilitating inflammatory skin disease, which mainly affects the inverse areas of the body leading to scarring and disfigurement (1, 2).
The European S1 guideline for the treatment of HS summarized all published treatments for HS (1). The quality of evidence for these treatments is generally low, as was recently demonstrated in a Cochrane Review on interventions for HS, which identified only 12 randomized controlled trials (RCTs) (3). Moreover, HS is a heterogeneous disease with distinct clinical phenotypes that may require different treatment strategies, further complicating the therapeutic decision-making process (4).
The European S1 guideline proposed a “Hurley severity grade-relevant treatment algorithm” (1). More recently Gulliver et al. (5) proposed another treatment algorithm based on disease severity measured by Hurley grade or PGA.
Hurley stage is a 3-stage classification of severity. Hurley stage I is characterized by abscess formation with-out sinus tracts and scarring. In Hurley II, patients have single or multiple separated areas of recurrent abscesses with sinus tracts and scarring, whereas in stage III the multiple interconnected sinus tracts and abscesses cover the whole affected anatomical area. This classification in its original form was created mainly for surgical purposes and does not take into account the inflammatory component. In addition, the extension of the disease, i.e. the number of anatomical areas involved, is not assessed. Accurate stratification of the wide variety of HS clinical phenotypes is therefore not possible with the original Hurley score.
Furthermore, the recently invented dynamic scoring system Hidradenitis Suppurativa Clinical Response (6) focuses mainly on the inflammatory component and is more or less comparable with a PASI 50 improvement in psoriasis and therefore is mainly suitable for the follow-up of systemic treatments. How-ever, these scores do not calculate or include the extensiveness of the disease. The number of anatomical areas involved is important in designing a holistic treatment plan as this should take into account the estimated number of surgical interventions needed (Fig. S1).
Here, we (the Dutch HS expert group and as a part of the European Hidradenitis Suppurativa Foundation e.V.) propose a refinement of the current Hurley staging.
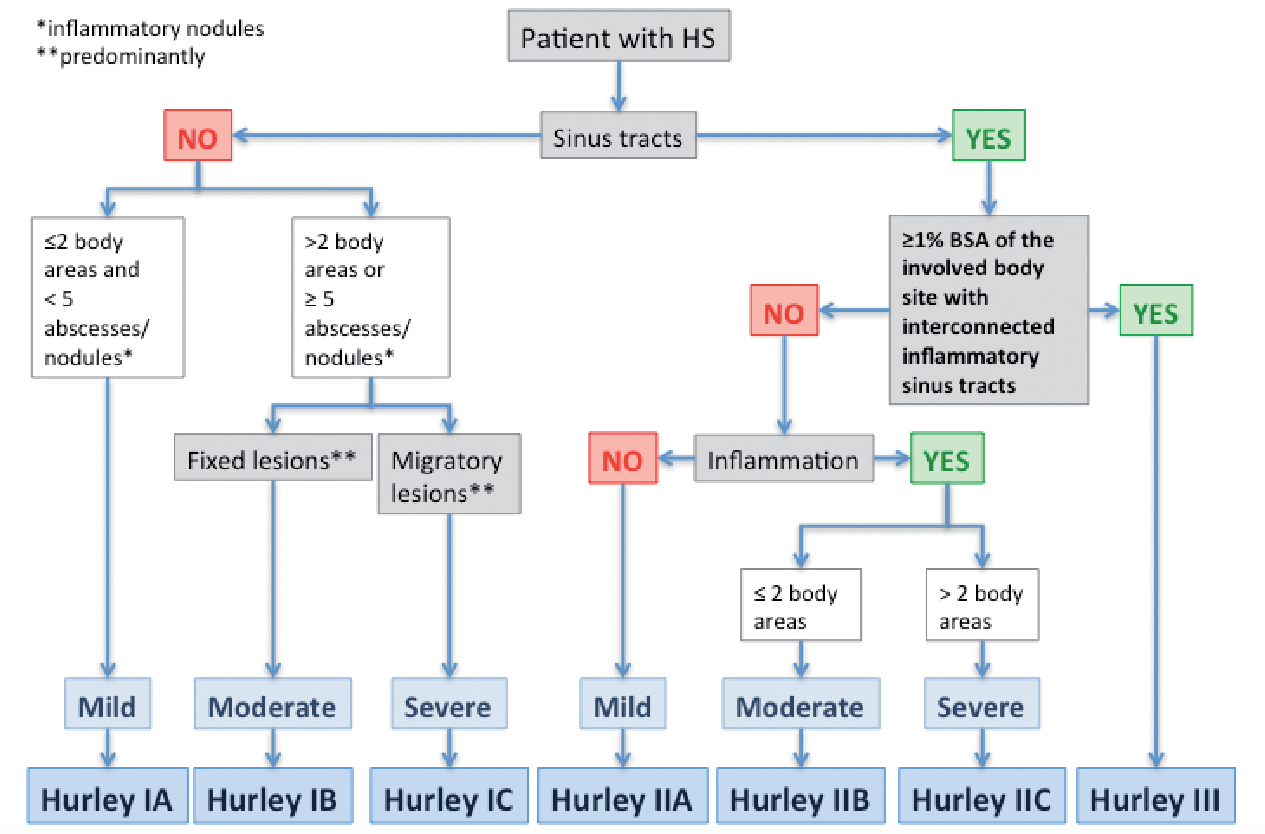
Briefly, a 3 stepwise algorithm, including assessing the presence of sinus tracts, degree of inflammation and the extensiveness, enables the clinician to assess severity across the different phenotypes of HS and helps to guide treatment (Fig. 1).
Fig. 1. Refinement of the Hurley classification: the 3-step algorithm. BSA: body surface area.
In the first step of the algorithm the presence of sinus tracts is assessed, clearly separating Hurley I from Hurley II and III. In Hurley I the differentiation between fixed and migratory lesions is essential. Hurley 1C is considered as severe HS and is characterized by the presence of migratory lesions and corresponds with the recently proposed scarring folliculitis and frictional furuncle phenotype (4). Since migratory lesions point to a strong inflammatory component, the cornerstone of treatment is anti-inflammatory agents rather than surgery. The difference between mild (A) and moderate (B) Hurley I is essential as it determines the extent of a potential surgical intervention.
Hurley stage II is characterized by the presence of sinus tracts and no longer by the presence of scarring, since this does not change the choice of treatment. In Hurley stage II the presence of inflammation (step 2), the extensiveness (step 3), whether 2 or more anatomical regions are involved, define the grade of severity and the choice of treatment (Fig. S2). In Hurley II without active inflammation, surgery is the first-line
therapy, whereas pre- or perioperative anti-inflammatory treatment should be considered when inflammation is present.
Hurley III is redefined as ≥ 1% body surface area (BSA) of a body site with interconnected inflammatory sinus tracts. In the original Hurley score an entire area must have been affected. In our view this refinement of Hurley III is necessary as there are large differences in surface size between anatomical areas; for example buttock vs. armpit.
In conclusion, our classification and the attached treatment ladder provide an easy way for clinicians to make a holistic therapeutic plan. First, it recognizes patients within Hurley I and II to have severe disease. Secondly, the definition of Hurley III is redefined as ≥1% BSA of a body site, to equalize the size of anatomical areas, which allows the earlier diagnosis of severe Hurley III in larger anatomical areas. The modifications help the clinician to guide therapy, especially in the choice between surgery and/or adjuvant anti-inflammatory drugs. Furthermore, the modifications provide the opportunity to prescribe anti-tumour necrosis factor (TNF) biologics for patients with Hurley stage 1C in whom surgery is not the appropriate option.
Conflicts of interest: BH has received an unrestricted educational grant and honoraria as a speaker and for participation on advisory boards from AbbVie, and received a research grant from Janssen Cilag B.V. (The Netherlands). BH performed investigator-initiated studies of Janssen-Cilag B.V. Furthermore, she acted as a consultant for AbbVie, Novartis, Pfizer and Mölnlycke. HvdZ has received honoraria from AbbVie for participation as a speaker and on advisory boards, and from Janssen for participation as a speaker. JB has received honoraria from AbbVie for participation on advisory boards. EP has received honoraria from AbbVie, Amgen, Celgene, Janssen, Galderma, Novartis and Pfizer for participation as a speaker, on advisory boards and received investigator-initiated grants (paid to the Erasmus MC) from AbbVie, AstraZeneca, Janssen, and Pfizer. RD has received honoraria from AbbVie and Galderma for participation on advisory boards and acted as a consultant for AbbVie and Galderma.


 Click to show fullsize
Click to show fullsize