


Departments of 1Dermatology, 2Hematology and 3Pathology, Hospital del Mar, Parc de Salut Mar, Passeig Marítim 25–29. ES-8003 Barcelona, Spain. E-mail: lidia.garcia.colmenero@gmail.com
Accepted Aug 16, 2016; Epub ahead of print Aug 18, 2016
Development of dystrophic xanthomatosis in cutaneous lesions of malignant haematological neoplasms is an uncommon phenomenon that has occasionally been reported in patients with primary cutaneous T-cell lym-phoma, especially in mycosis fungoides (1–3) and CD30+ cutaneous lymphoproliferative disorders (4, 5). In such diseases, xanthomatization of lesions most commonly occurs in regressing skin tumours or plaques after initiation of treatment, and is histologically characterized by a diffuse dermal infiltration of lipid-laden macrophages sometimes associated with persistent atypical lymphoid cells. To our knowledge, no previous reports of xanthomatous changes have been reported in regressing skin lesions of blastic plasmacytoid dendritic cell neoplasm (BPDCN).
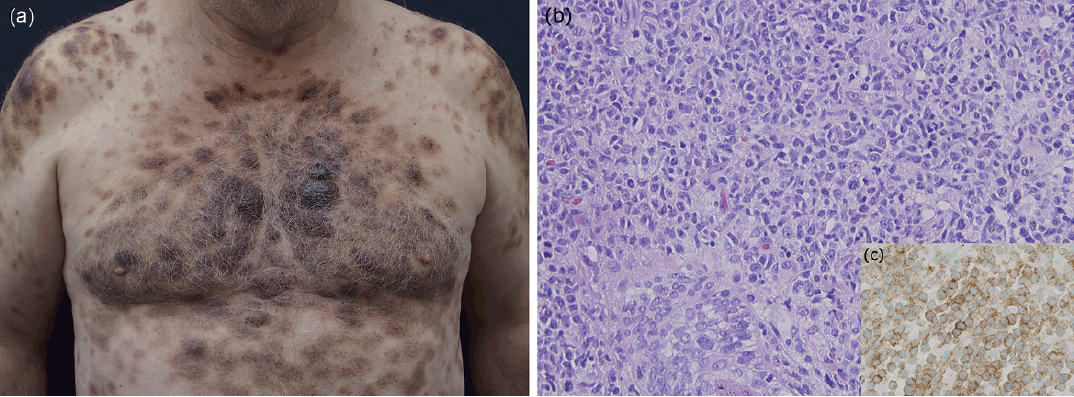
A 61-year-old man with a personal history of hypo-thyroidism treated with levothyroxine was referred for evaluation of multiple papulo-nodules that had appeared progressively on the scalp and trunk over the last 2 months. Physical examination disclosed multiple well-demarcated, firm, non-ulcerated, 0.5–4 cm diameter, dark-purple nodules with a bruise-like appearance involving most of the surface of his scalp and trunk (Fig. 1a). No peripheral enlarged lymph nodes were identified. Laboratory investigations revealed anaemia (Hb 110 g/l), leukopaenia (3,300/μl), neutropaenia (660/μl) and thrombocytopaenia (108,000/μl). No alterations in lipid metabolism, lactate dehydrogenase and beta 2-microglobulin were detected.
Fig. 1. (a) Initial presentation of blastic plasmacytoid dendritic cell neoplasm. Bruise-like tumefactions on the trunk and arms. (b) Diffuse dermal infiltrate by medium to large-sized round to oval blast-like cells. Haematoxylin and eosin (HE) ×200 (c) The atypical cells were positive for the CD123 antigen. CD123 ×400.
Skin biopsy showed a non-epidermotropic, diffuse dermal infiltrate composed of medium-to-large-sized round-to-oval blast-like cells (Fig. 1b). Immunohisto-chemical staining revealed that these atypical cells expressed CD4, CD56 and CD123 (Fig. 1c), and were negative for B (PAX5, CD20) and T-cell markers (CD3, CD5, CD7, CD8), as well as TdT, CD34, myeloperoxidase (MPO), CD68 and in situ hybridization for Epstein-Barr virus-encoded mRNA (EBERs). Ki67 labelling index was 40%. Bone marrow biopsy showed infiltration by atypical cells with an identical phenotype as those observed in the skin. Peripheral blood involvement was not detected. After a full-body computed tomography (CT) scan, which revealed no abnormalities, a diagnosis of blastic plasmacytoid dendritic cell neoplasm with cutaneous and bone marrow involvement was established.
Treatment with chemotherapy, consisting of vincristine, daunorubicin, L-asparaginase and prednisone (schedule LAL-RI-08 for acute lymphoblastic leukaemia), was started. Following the first course of chemotherapy, the nodules decreased in size significantly and some of them adopted a yellowish coloration (Fig. 2a). A biopsy specimen obtained from a yellowish plaque showed mild dermal perivascular lymphoid infiltrates admixed with clusters of foamy histiocytic cells with no evidence of atypical residual cells (Fig. 2b). Bone marrow biopsy demonstrated the absence of neoplastic cells, and complete remission was confirmed. No recurrence of cutaneous lesions was observed after 4 months of follow-up.
Fig. 2. (a) Yellowish discoloration of the previously affected sites after specific chemotherapy. (b) Clusters of foamy histiocytes. Haematoxylin and eosin ×400.
Dystrophic xanthomatization defines the accumulation of lipid-rich foam cells within an area of damaged skin, both in normolipaemic or hyperlipoproteinaemic states. This is an uncommon phenomenon that may develop in a wide spectrum of local inflammatory (recurrent phlebitis and lymphangitis, photosensitivity disorders, exfoliative erythroderma, herpes zoster), non-inflammatory (lymphoedema, trauma) and neoplastic diseases (breast carcinoma) (6) that may trigger stimuli leading to secondary lipid deposition. The pathogenic mechanisms behind the development of dystrophic xanthomas in cutaneous haematological diseases are not well-understood. Lipids are probably released from neoplastic cells after local tissue hypermetabolism or damage following therapy, and therefore engulfed by macrophages (7). In addition, it has been hypothesized that a release of intracytoplasmic cytokines, such as interleukin-4 (8), could directly activate the histiocytic response and, in rare instances, malignant cells may play a direct role in lipoprotein processing and xanthomatization (9).
The association of secondary xanthomatization in malignant haematological disorders other than primary cutaneous T-cell lymphomas is a rare phenomenon. Isolated reports of cutaneous dystrophic xanthomatosis developing in specific cutaneous lesions of patients with Sézary syndrome, adult T-cell leukaemia/lymphoma or chronic myelomonocytic leukaemia (10) have been reported previously. This phenomenon has also been described in association with Burkitt’s lymphoma of the small intestine (11). Xanthomatous changes in cutaneous lesions of blastic plasmacytoid dendritic cell neoplasm after specific chemotherapy are reported here for the first time. Therefore, blastic plasmacytoid dendritic cell neoplasm should be added to the list of disorders in which the phenomenon of cutaneous dystrophic xantho-matization in regressing lesions after treatment has been observed.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize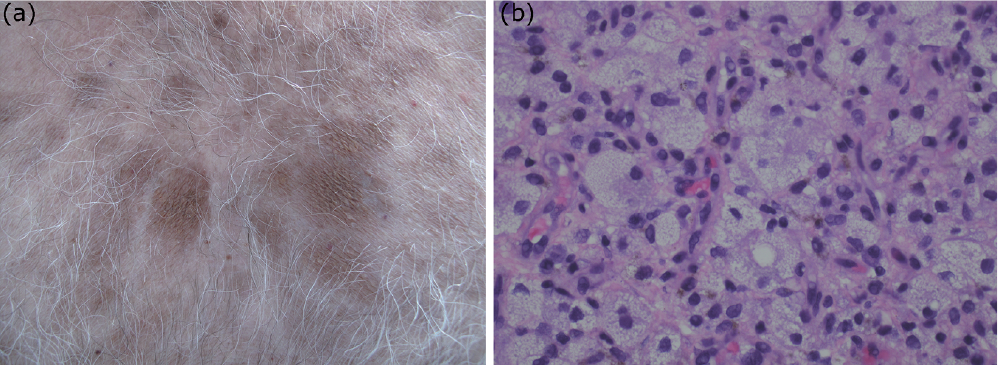 Click to show fullsize
Click to show fullsize